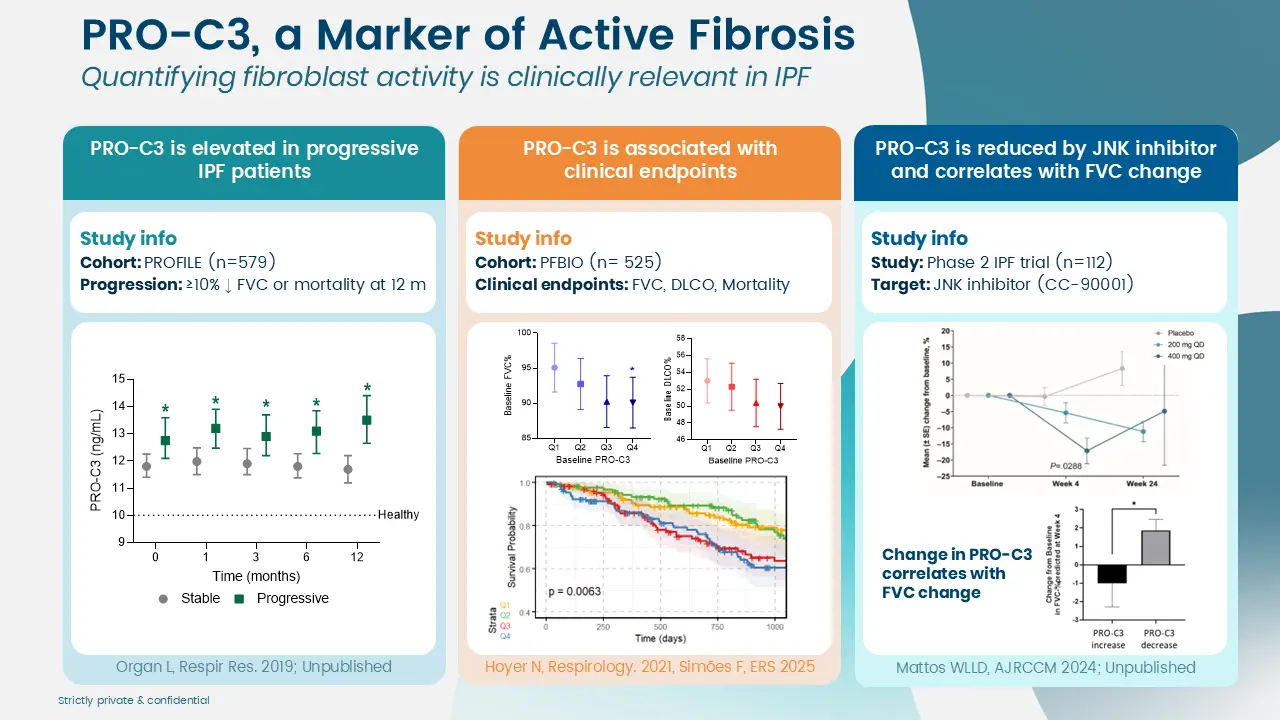
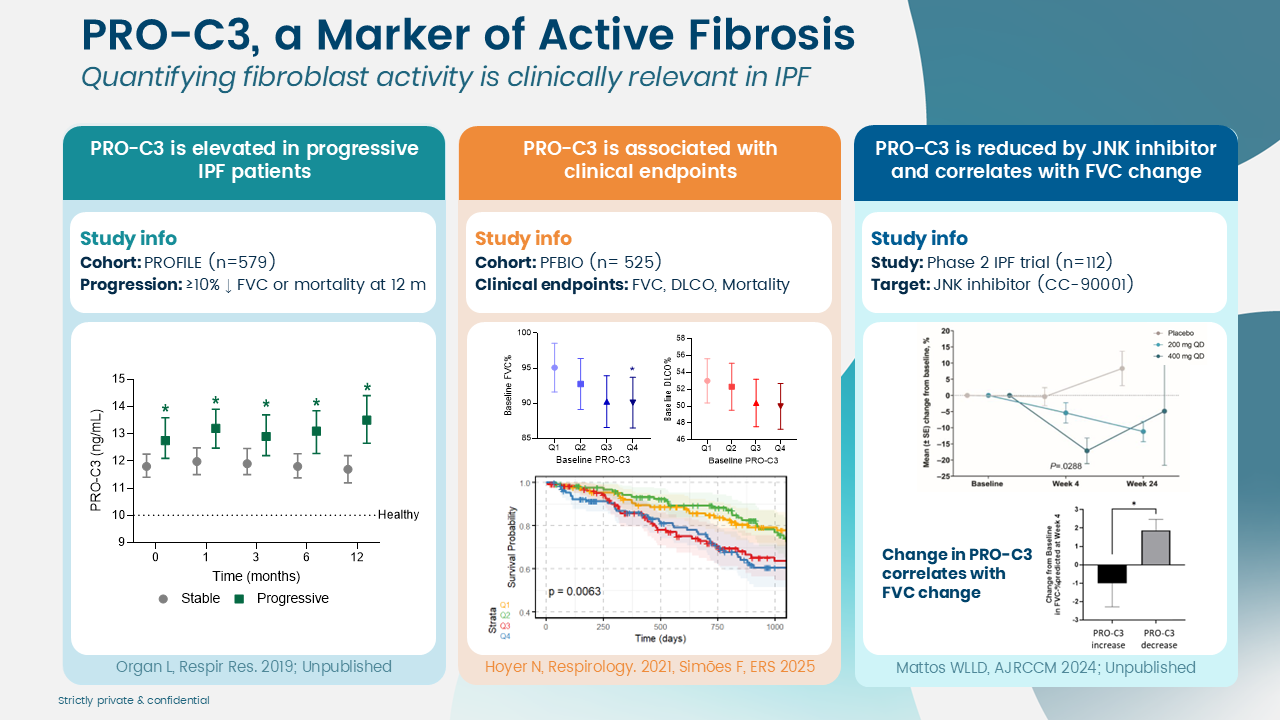
Extracellular matrix (ECM) remodeling is a central driver of disease progression in idiopathic pulmonary fibrosis (IPF) and other ILDs. At the cellular level, these remodeling processes ultimately lead to the decline in lung function seen in patients.
For drug developers, this means that modifying ECM remodeling is a key therapeutic objective.
But to evaluate whether novel compounds are working, we need reliable tools that measure the biological processes driving the disease.
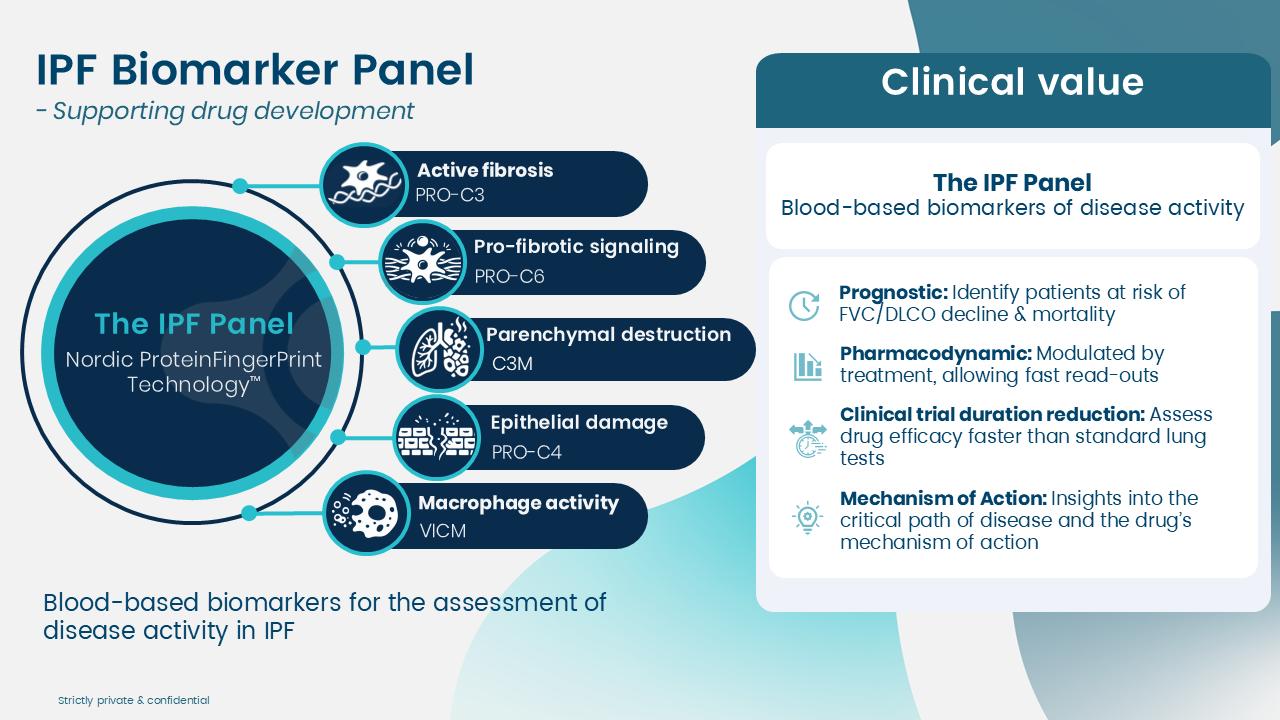
We have developed a panel of ECM remodeling biomarkers based on our ProteinFingerprint Technology™ and 30 years of biomarker expertise.
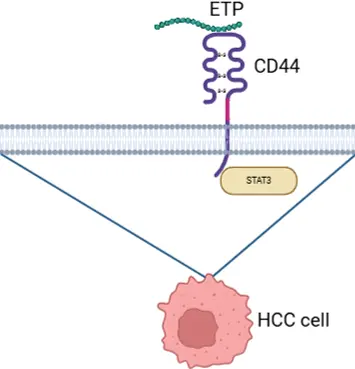
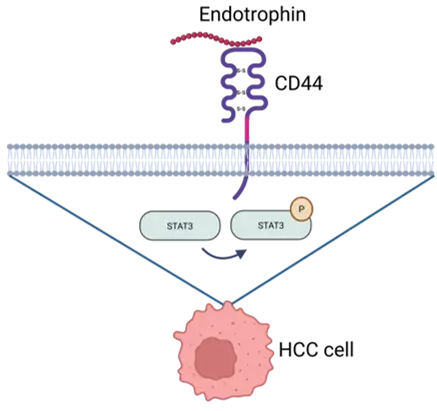
For years, Endotrophin has been discussed as a circulating signal linked to fibroinflammatory disease severity and adverse outcomes. But there has been a persistent gap between association and a clearly defined, targetable mechanism. Now, a new report addresses that gap by identifying CD44 as a receptor for Endotrophin and connecting Endotrophin–CD44 binding to STAT3 signaling in hepatocellular carcinoma (HCC).
This publication anchors that association mechanistically by showing that Endotrophin is produced in fibrotic liver by COL6A3‑rich hepatic stellate cells (HSCs) and is not merely a degradation product, but a bioactive hormone-like peptide that signals into neighboring cells.
In the study’s experimental system, Endotrophin binding to CD44 activated STAT3 signaling and was linked to phenotypes relevant to tumor progression, including epithelial–mesenchymal transition (EMT), proliferation, and sorafenib resistance.
Fibroblast-derived Endotrophin signals into CD44+ cells and sustains itself
The paper further describes that hepatic stellate cell–derived Endotrophin targets pericentral CD44+ tumor cells, induces COL6A3 expression, and sustains Endotrophin production via a STAT3-dependent feedback loop.
Schematic of Endotrophin binding to CD44 and downstream STAT3 signaling. Created in BioRender. Gongora, F. (2026) https://BioRender.com/juay2se
When the Endotrophin-CD44 axis is activated, Endotrophin/PRO-C6 can serve as target engagement or stratification tools. Created in BioRender. Laursen, C. (2026) https://BioRender.com/2kd3vyi
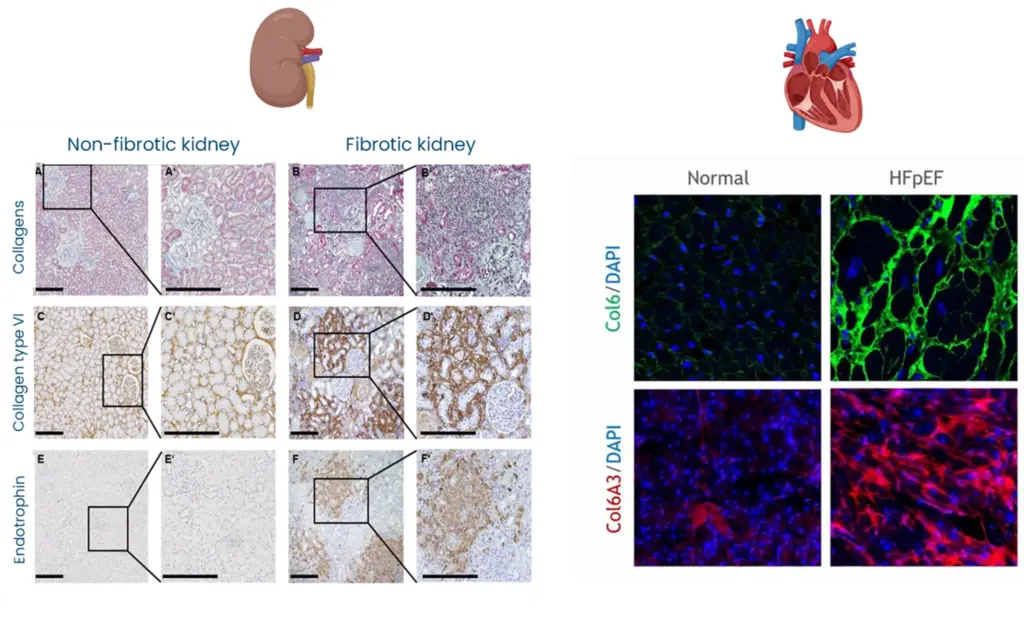
By defining CD44–STAT3 as the principal Endotrophin signaling route in HCC, the paper suggests a shared signaling logic by which Endotrophin‑rich fibrotic niches (kidney, heart, adipose tissue) can drive organ damage and risk of outcome through similar downstream pathways.
Interested in how Endotrophin relate to fibroblast activity?
Circulating Endotrophin likely reflects an activated Endotrophin-CD44–STAT3 loop in fibrotic organs. High circulating Endotrophin is not only a marker of fibroblast activity but a surrogate for an ongoing pathogenic signaling circuit. Inhibiting the Endotrophin–CD44–STAT3 axis (genetic Col6a3/Cd44 deletion, STAT3 inhibition, or CD44‑binding‑defective Endotrophin mutants) attenuates fibrosis, EMT, steatosis and chemoresistance, positioning this axis as a therapeutic target in metabolic dysfunction-associated HCC.
Endotrophin‑rich fibrotic niches can drive organ damage and risk of outcome
Endotrophin does not only stage and prognosticate fibrotic disease but can also identify patients in whom Endotrophin‑driven fibro-inflammatory signaling is active and may be actionable by Endotrophin‑neutralizing antibodies or STAT3‑targeted interventions.
Why measure outcomes and risk signals across chronic disease
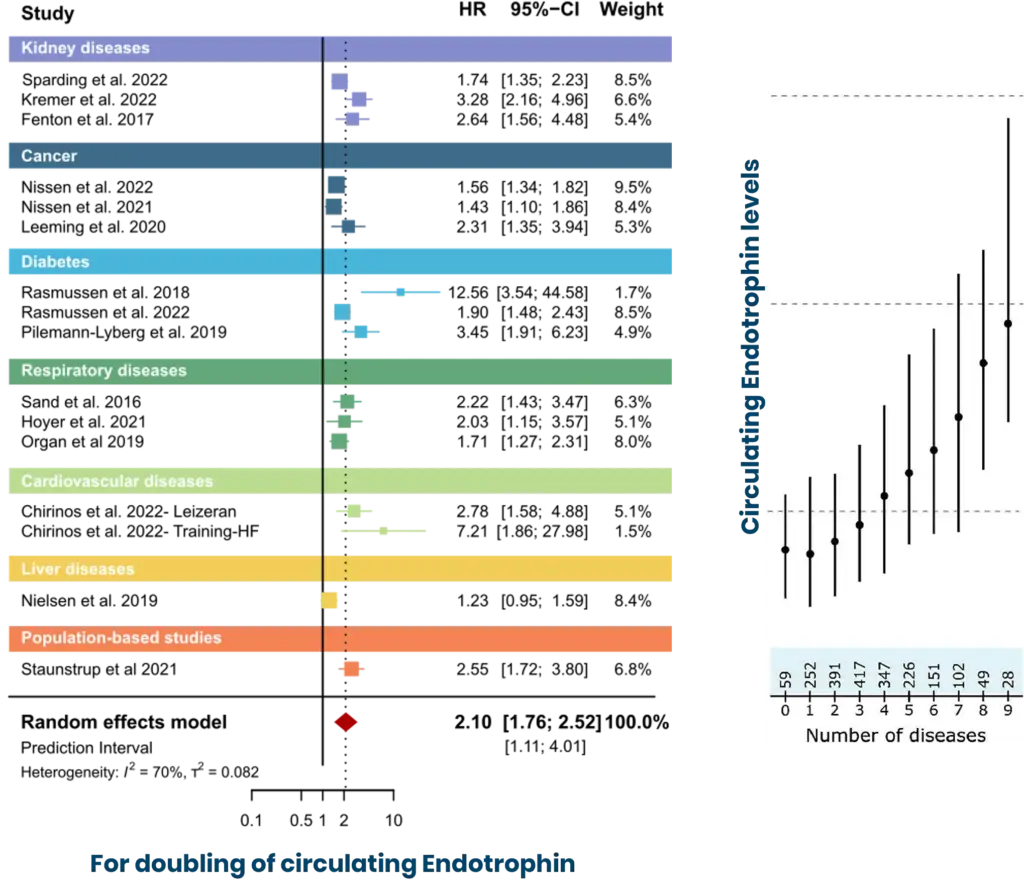
Endotrophin in the blood reflects fibro-inflammatory remodeling associates with cardiac and kidney fibrosis, mortality, and progression of MASH, cirrhosis, and HCC, with levels rising across the spectrum of metabolic diseases.
Endotrophin is not just “another fibrosis marker,” but a circulating readout of active fibro-inflammatory biology. In a systematic review and individual participant data meta-analysis, higher circulating Endotrophin independently associated with increased mortality risk across a broad range of chronic diseases: a core clinical reason to measure Endotrophin and nordicPRO-C6™ in programs where baseline biology and outcome risk need to be quantified.
Mechanistically, Endotrophin upregulates and releases into circulation as a consequence of recurring pathophysiological mechanisms across diseases. The functional implication of circulating Endotrophin supports PRO-C6 as an operational biomarker in clinical programs, where a blood-based measurement aligned with fibroblast-driven remodeling biology can be used at scale and longitudinally.
How does CD44 connect to existing literature on Endotrophin?
The new receptor paper changes how to interpret associations by providing a defined signaling handle. CD44 was identified as an Endotrophin receptor, and Endotrophin–CD44 engagement activated STAT3 signaling with disease-relevant phenotypes. When a circulating molecule is both outcome-associated and connected to a receptor axis, measuring Endotrophin and PRO-C6 becomes a practical component of biology-aware stratification and monitoring in fibro-inflammatory clinical programs. Nordic’s measurement approach centers on assays that quantify Endotrophin-related biology in circulation, including PRO-C6-based measurement supported through clinical evidence.
If your program involves fibro-inflammatory biology, position Endotrophin measurement as an evidence-aligned readout to support:
Baseline characterization of fibroblast-associated signaling burden,
Risk stratification informed by published outcome associations across chronic disease,
Mechanistic hypothesis testing in settings where CD44/STAT3 biology is part of the rationale.
A recent analysis published in JAMA highlights a major epidemiological shift: Colorectal cancer (CRC) is now the leading cause of cancer-related death among adults under 50 in the United States.
CRC has long been perceived as a disease of older populations. The rapid rise in early-onset cases challenges that assumption and reinforces the need to rethink both biology and treatment strategies.
Why standard therapies still fall short: the fibrotic stroma as a resistance mechanism
Therapeutically, the backbone remains surgery in localized disease, combination chemotherapy regimens such as FOLFOX and FOLFIRI, anti-VEGF or anti-EGFR targeted therapies in selected patients, and immunotherapy in MSI-high/dMMR tumors. While these approaches have extended survival, resistance and relapse remain frequent, particularly in advanced disease.
One key and often underestimated driver of progression and resistance is fibrosis. CRC tumors are embedded in a collagen-rich, fibrostenotic microenvironment shaped by cancer-associated fibroblasts (CAFs). This dense extracellular matrix (ECM) does not merely provide structure. It represents a desmoplastic barrier that limits drug penetration, reduces treatment efficacy, and supports tumor progression.
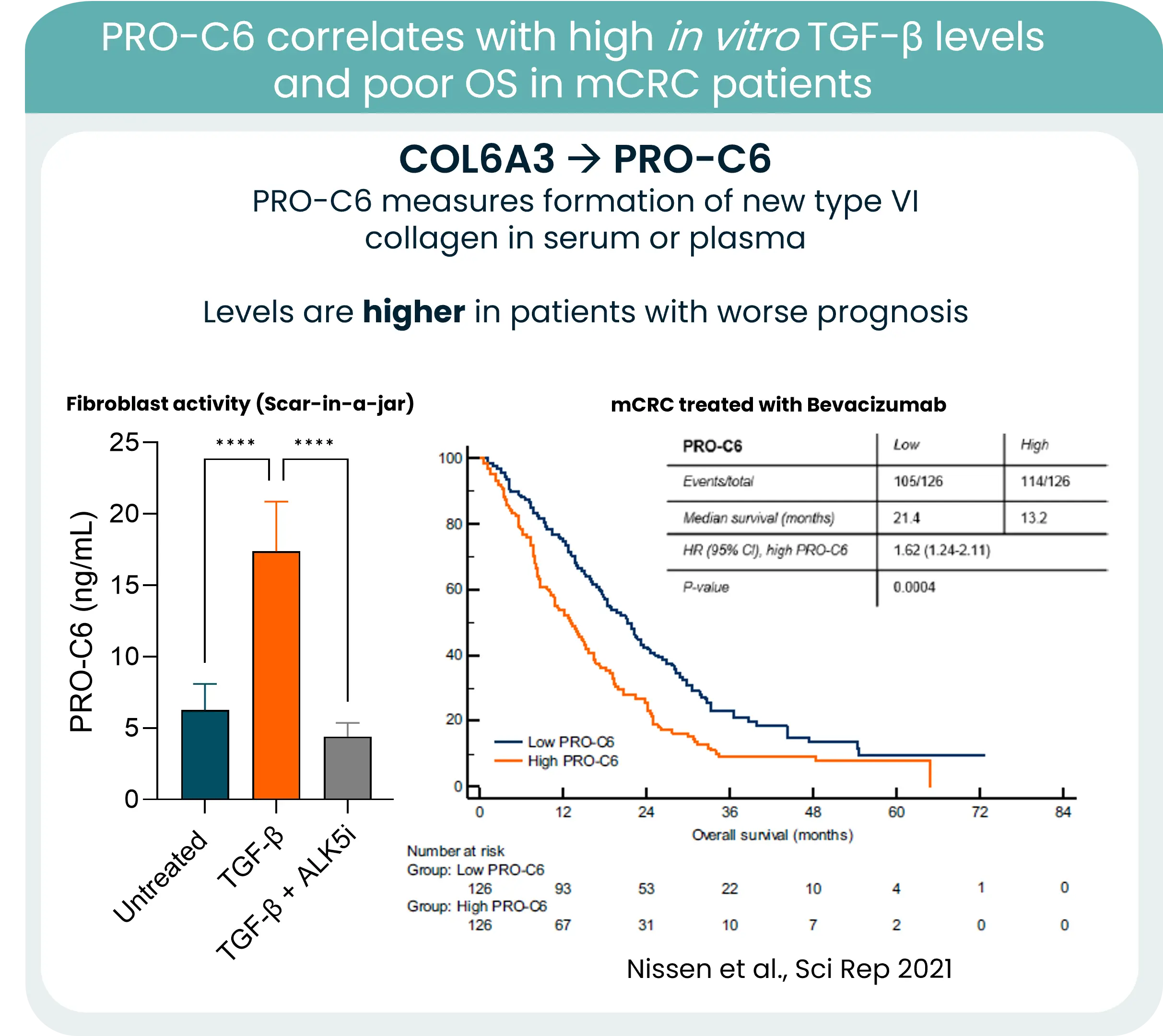
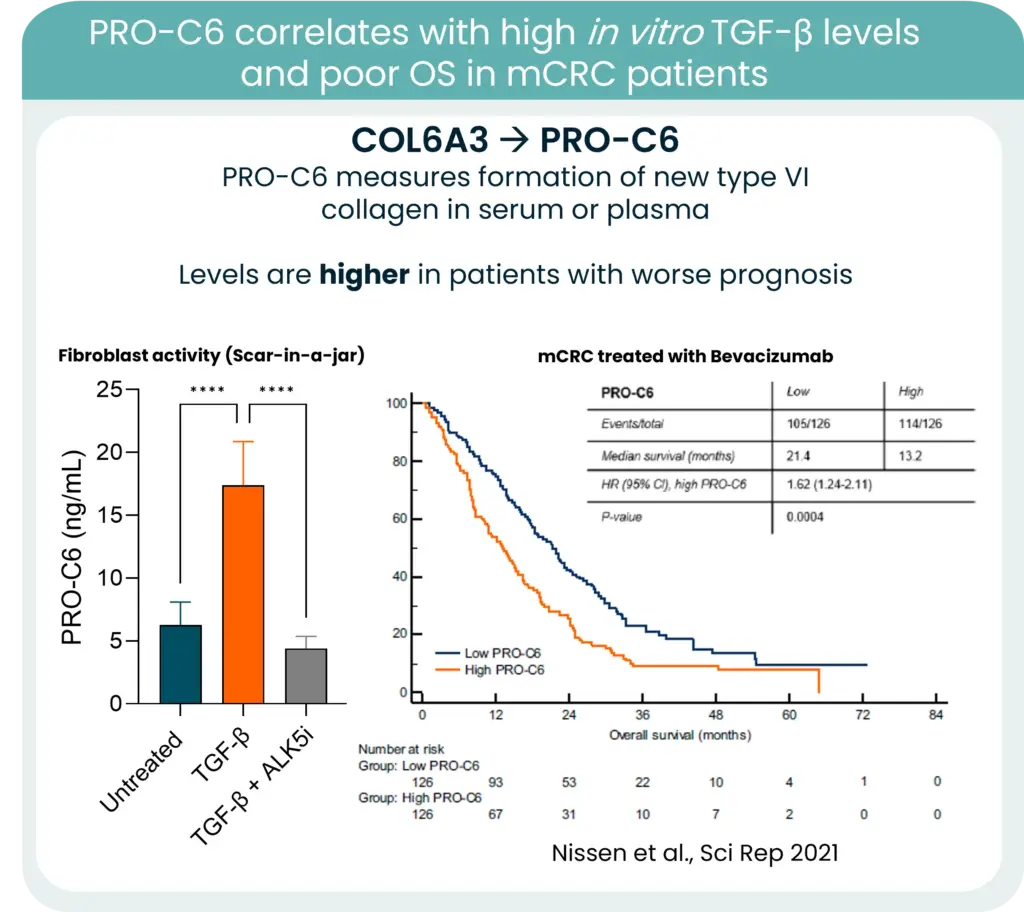
PRO-C6 correlates with TGF-β levels and overall survive in mCRC patients
From biology to measurement: collagen remodeling biomarkers
Collagens are central components of this barrier, and increased collagen deposition and remodeling consistently associate with poorer outcomes. One notable example is type VI collagen. Its gene expression is strongly associated with KRAS mutations and high TGF-β levels in CRC. New type VI collagen formation releases protein fragments to the bloodstream, which can be quantified in serum using our PRO-C6 biomarker and correlate to high TGF-β levels and poor OS.
In this context, measuring collagen formation and degradation becomes highly relevant. Quantifying ECM remodeling can provide insight into tumor aggressiveness, stromal activation, and potentially treatment response.
As early-onset CRC continues to rise, integrating stromal blood-based biomarkers into clinical strategy may refine risk stratification and open new opportunities for stroma-targeted interventions.
The future of CRC management will not rely solely on targeting tumor cells. It will require understanding and measuring the fibrotic environment that sustains them.
Nordic Bioscience´s neurology team has had 4 abstracts and oral presentation accepted at the AD/PD™ Alzheimer’s Disease and Parkinson’s Disease Conference in 2026.
The abstracts cover the following topics:
Modulation of blood-brain barrier integrity biomarkers in neurological disorders
Upregulation of serum calprotectin biomarkers in patients with Parkinson’s Disease
Elevation of type III and IV collagen fragments in the serum of treatment naïve multiple sclerosis patients
Biomarker profiling for the diagnosis of Parkinson’s disease
Alzheimer’s Disease, Multiple Sclerosis and Parkinson’s Disease are neurological disorders with devastating consequences for those affected and their families. These diseases are characterized by a lack of biomarkers specifically tracking disease progression and the effect of potential disease modifying therapies, leading to inadequate treatment possibilities and patient care.
In Alzheimer’s Disease (AD), recently developed fluid biomarkers, such as phospho-Tau isoforms (pTau217), have shown the ability to predict disease progression and treatment response in both plasma and CSF (measured in our CAP/CLIA-certified lab). This clearly illustrates how far the neuro field has come and highlights the importance of such biomarkers or continuous drug development in AD.
For Multiple Sclerosis (MS) and Parkinson’s Disease (PD), the work focuses on identifying a panel of biomarkers reflecting different aspects of these complex diseases, including neuroinflammation, blood-brain barrier integrity and active neurodegeneration.
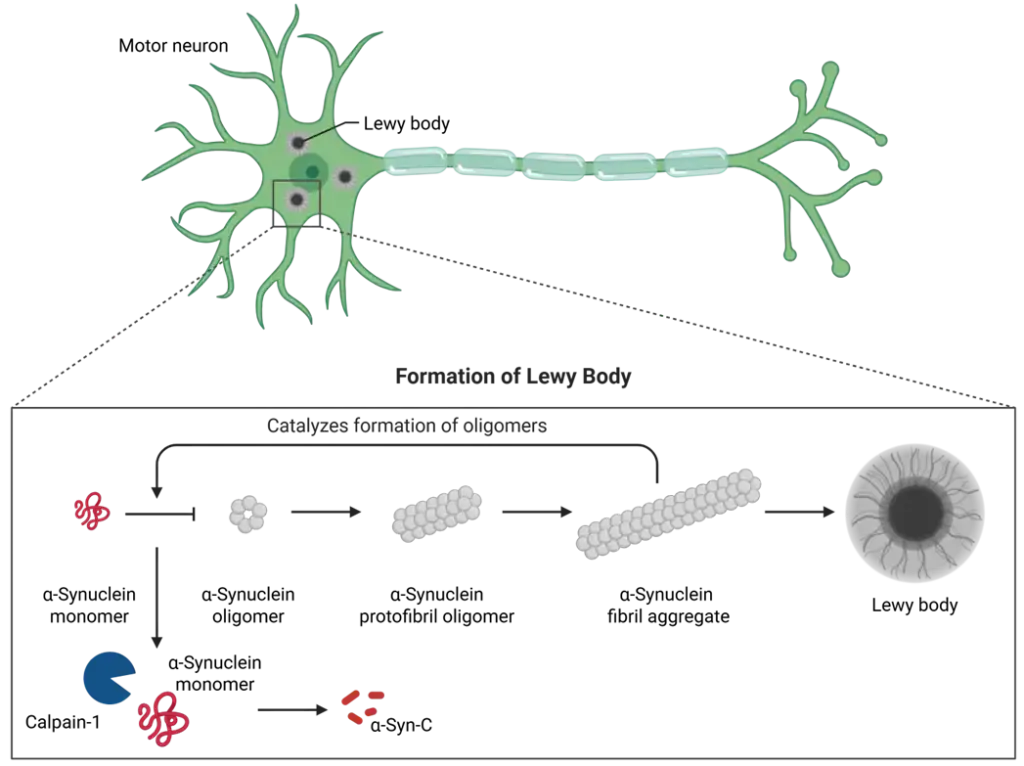
From pTau217 to α-Synuclein: New Biomarkers Driving Neurodegeneration and Neuroinflammation Research
There are therapies and biomarkers available in MS, but we still lack refined biomarkers to monitor the ongoing efficacy of the drugs. Such biomarkers can be used to enrich patient populations with respect to responses, as well as supporting the development of new drugs. Biomarkers such as fragments of collagen type IV, which reflect turnover of the basement membrane of the blood-brain barrier, have shown promise.
At the same time, in PD, there is a lack of biomarkers reflecting the underlying neuronal pathology especially in plasma/serum. Consequently, there is a competition on being the first to robustly detect the key protein α-synuclein—a biomarker that can capture the underlying pathology. Here, we introduced a novel assay detecting fragments of α-synuclein, which are generated during the loss of neurons. After further investigation, this biomarker could potentially become an important tool for drug development in PD.
Overall, fluid biomarkers for neurodegenerative diseases have come a long way in the last decade and are clearly critical to the success of drug development trials.
TGFβ signaling: a game changer in personalized cancer treatments?
Treatment outcomes are deeply influenced by the tumor microenvironment (TME) where TGFβ (Transforming Growth Factor Beta) has emerged as a critical factor that can dictate the success—or failure—of therapeutic strategies.
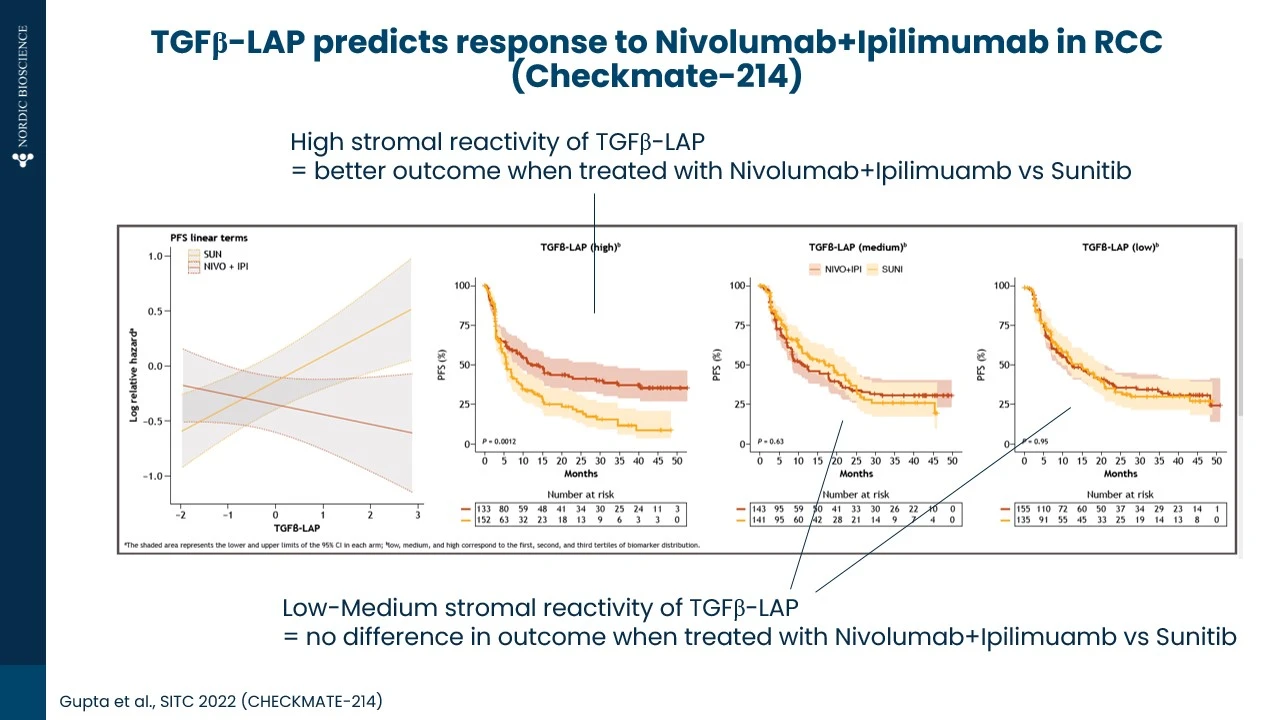
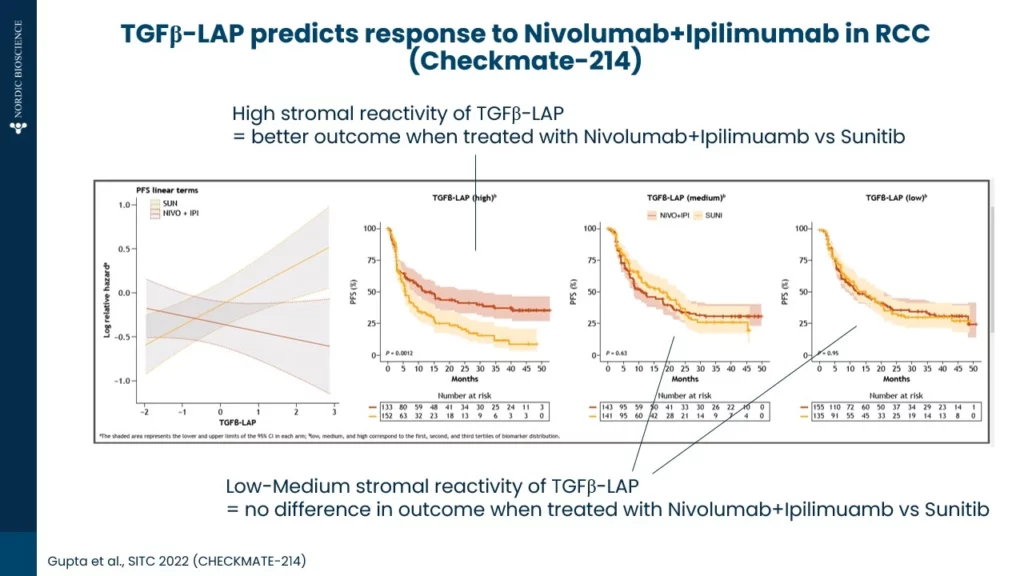
As shown below (Figure 1.) in an example from renal cell carcinoma (RCC), high TGFβ activity contributes to poor responses to tyrosine kinase inhibitors (TKIs) as compared immune checkpoint inhibitors. TGFβ activity was measured by the TGFβ-LAP biomarker in pre-treatment serum.
Conventional TGFβ assays are affected by platelets releasing TGFβ during clotting (drastically affecting the measurements in serum). In contrast, the TGFβ-LAP biomarker quantifies a cleaved latent activating protein (LAP) fragment which is independent of platelet TGFβ release providing a novel tool to indirectly measure TGFβ in serum.
Figure 1.TGFβ (Transforming Growth Factor Beta) has emerged as a critical factor that can indicate success rate
Why does this happen?
TKIs, such as Sunitinib, are primarily targeting angiogenesis and signaling pathways critical for tumor growth. However, elevated TGFβ promotes an immunosuppressive and fibrotic TME, counteracting these therapies by enhancing tumor resilience and protecting vasculature from the intended effects of TKIs. On the other hand, anti-PD-1/anti-CTLA-4 immuno-oncology (IO) therapies such as Nivolumab and Ipilimumab, which aim to re-activate T-cell responses, may be relatively more effective even in a TGFβ-rich environment.
Personalizing treatment (TKI vs. IO) with biomarker-driven approaches
Understanding TGFβ activity could be a game-changer in personalizing cancer treatments. Biomarkers that measure TGFβ levels or its downstream effects might help clinicians choose between TKIs or immunotherapy – or even better, design combination regimens. This underscores the importance of a biomarker-driven approach to cancer treatments. As we continue to unravel these mechanisms, the goal remains clear: to turn the TME from a shield into a target.
Our approach is designed to be implemented into clinical trials and research programs on TKI vs. IO, and to help explore the intersection of TGFβ biology and therapeutic resistance.