CPa9-HNE ELISA has emerged as a novel serum calprotectin biomarker
Status quo: Crohn’s and Colitis biomarkers
Conventional serum calprotectin biomarkers are often not as clinically useful as the fecal versions, which is related to the half-life of calprotectin in blood (only 5-6 hours), leading to dissociation of calprotectin protein. The short half-life of calprotectin in blood reduces the window in which the current serum calprotectin ELISA assay can detect calprotectin dimer protein, which is composed of monomers S100A8 and S100A9.
By applying the Protein Fingerprint technology, we have identified a neo-epitope of the S100A9 monomer of calprotectin derived from proteolytic cleavage by human neutrophil elastase (HNE). This ELISA assay is referred to as the CPa9-HNE (nordicCPa9™) assay and is a new and innovative method for quantification of calprotectin in serum developed by Nordic Bioscience.

A new tool to measure… calprotectin
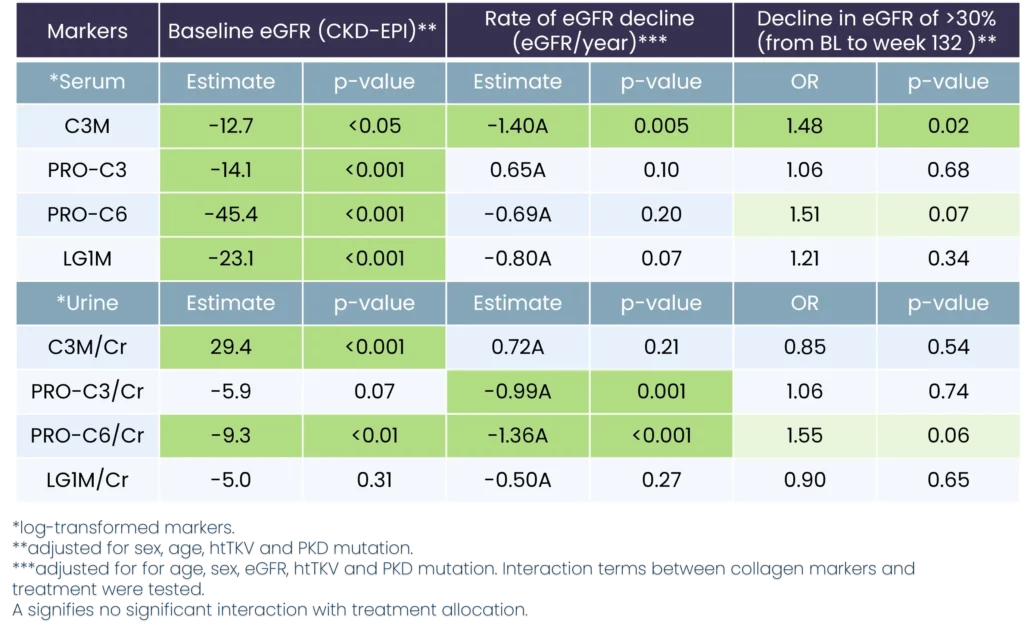
Patients with Crohn’s disease and ulcerative colitis have been found to show significantly higher levels of CPa9-HNE (nordicCPa9™) in their serum than healthy subjects, with the AUC reaching 0.98 (CI: 0.97-1.00, p<0.0001) for CD and 0.96 (CI: 0.92-1.00, p<0.0001) for UC, proving the assay’s efficacy in distinguishing between disease states.
In comparison, the MRP8/14 serum calprotectin assay from Bühlmann Lab, while also used to identify IBD, showed poorer separation between patients and healthy subjects, with AUCs of 0.72 (CI: 0.59-0.86, p=0.0025) for UC and 0.70 (CI: 0.56-0.84, p=0.0046) for CD, respectively.
The nordicCPa9™ biomarker showed a better correlation with the endoscopic score for Crohn’s disease (SES-CD) and ulcerative colitis (MES) than the FCP. At the same time, the MRP8/14 assay and neutrophil count showed no significant correlation with endoscopic scores for IBD patients.
To investigate the accuracy of the nordicCPa9™, we performed a received operator characteristic curve, demonstrating nordicCPa9™ with acceptable accuracy to identify patients with IBD in remission vs. active disease.
Finally, we demonstrated that the nordicCPa9™ biomarker could detect the calprotectin neo-epitope only in the supernatant of in vitro activated primary human neutrophils, but not in inactive primary human neutrophils. This was in contrast to the MRP8/14 serum CP assay of the Bühlmann lab, as both inactive and activated primary human neutrophils secreted detectable levels of calprotectin.
NordicCPa9™ ELISA proved to be a novel serum calprotectin biomarker with significant clinical potential as a biomarker for patients with IBD to monitor disease activity and neutrophil activity.
However, circulating calprotectin metabolites released from locally inflamed mucosa are not be dissociated further. They can be readily quantified using an ELISA-based technique called Protein Fingerprint technology. This refined ELISA technique quantifies protein metabolites or neo-epitopes derived from proteolysis that reflect local tissue inflammation and remodeling.