TGFβ signaling: a game changer in personalized cancer treatments?
Treatment outcomes are deeply influenced by the tumor microenvironment (TME) where TGFβ (Transforming Growth Factor Beta) has emerged as a critical factor that can dictate the success—or failure—of therapeutic strategies.
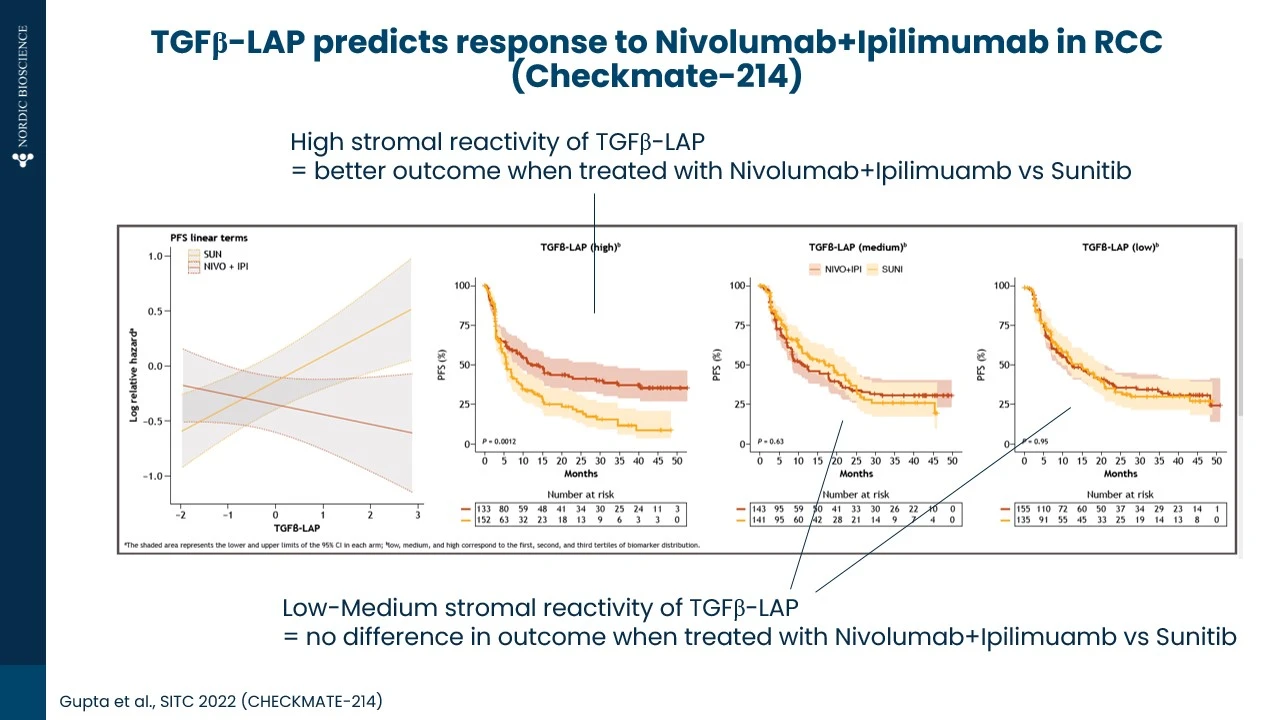
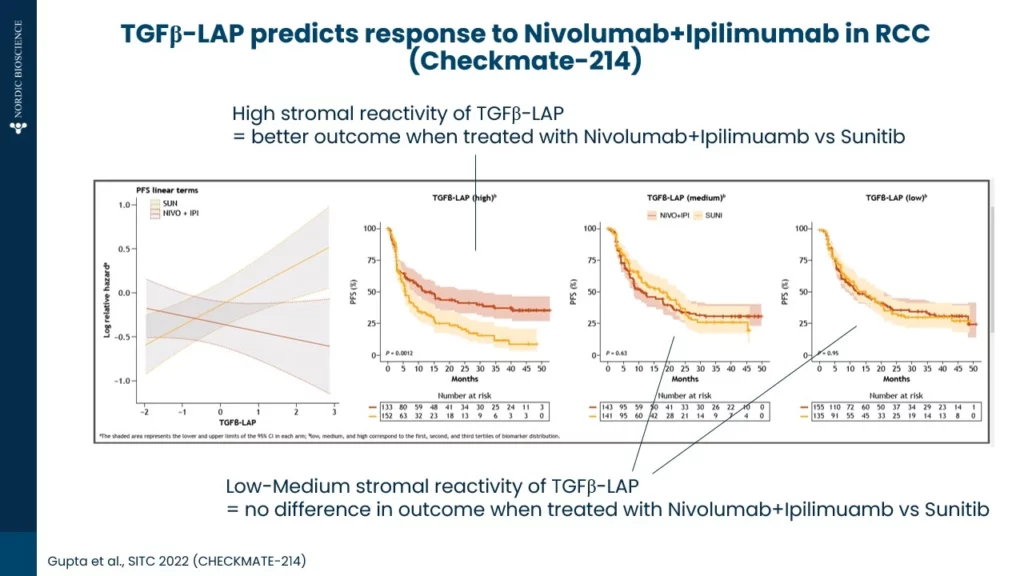
As shown below (Figure 1.) in an example from renal cell carcinoma (RCC), high TGFβ activity contributes to poor responses to tyrosine kinase inhibitors (TKIs) as compared immune checkpoint inhibitors. TGFβ activity was measured by the TGFβ-LAP biomarker in pre-treatment serum.
Conventional TGFβ assays are affected by platelets releasing TGFβ during clotting (drastically affecting the measurements in serum). In contrast, the TGFβ-LAP biomarker quantifies a cleaved latent activating protein (LAP) fragment which is independent of platelet TGFβ release providing a novel tool to indirectly measure TGFβ in serum.
Figure 1.TGFβ (Transforming Growth Factor Beta) has emerged as a critical factor that can indicate success rate
Why does this happen?
TKIs, such as Sunitinib, are primarily targeting angiogenesis and signaling pathways critical for tumor growth. However, elevated TGFβ promotes an immunosuppressive and fibrotic TME, counteracting these therapies by enhancing tumor resilience and protecting vasculature from the intended effects of TKIs. On the other hand, anti-PD-1/anti-CTLA-4 immuno-oncology (IO) therapies such as Nivolumab and Ipilimumab, which aim to re-activate T-cell responses, may be relatively more effective even in a TGFβ-rich environment.
Personalizing treatment (TKI vs. IO) with biomarker-driven approaches
Understanding TGFβ activity could be a game-changer in personalizing cancer treatments. Biomarkers that measure TGFβ levels or its downstream effects might help clinicians choose between TKIs or immunotherapy – or even better, design combination regimens. This underscores the importance of a biomarker-driven approach to cancer treatments. As we continue to unravel these mechanisms, the goal remains clear: to turn the TME from a shield into a target.
Our approach is designed to be implemented into clinical trials and research programs on TKI vs. IO, and to help explore the intersection of TGFβ biology and therapeutic resistance.
Understanding Parkinson’s Disease Progression Through Protein Biomarkers
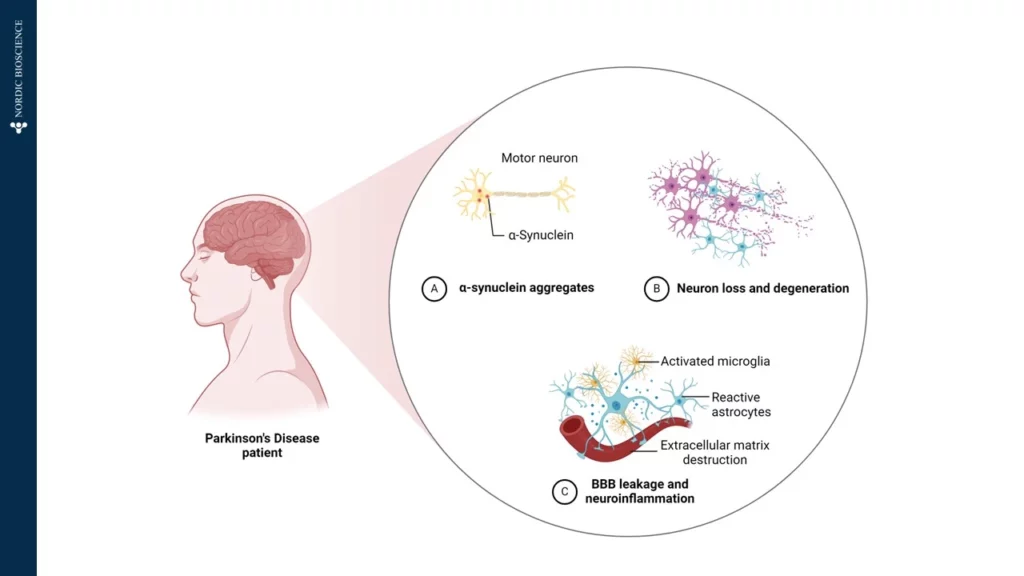
Parkinson’s Disease (PD) is a complex neurodegenerative disorder, primarily affecting the brain’s control over movement, thought, memory, and emotion. Early symptoms often manifest as tremors due to impaired motor skills. Underlying these visible symptoms is a cascade of molecular changes, beginning with alterations in specific proteins—one of which, α-synuclein, plays a critical role in PD pathology. In Figure 1, we have illustrated how α-Synuclein aggregates, which impairs the motor neuron.
Figure 1.Patients diagnosed with Parkinson’s Disease is affected by A) α-Synuclein aggregates affecting the motor neurons, B) Neuron loss and degeneration, and C) Blood-Brain-Barrier (BBB) leakage and neuroinflammation, by activated microglia, reactive astrocytes and extracellular matrix destruction.
In a healthy brain, α-synuclein supports neuronal communication. However, in Parkinson’s, this protein undergoes abnormal processing, driven partly by the enzyme Calpain-1, which cleaves α-synuclein into smaller, altered fragments. This early cleavage disrupts cellular function and promotes the formation of toxic aggregates, which accumulate, kill neurons, and drive disease progression. Intriguingly, these fragmented proteins can cross the blood-brain barrier and enter the bloodstream, providing a potential “window into the brain” for tracking disease activity from a simple blood sample.
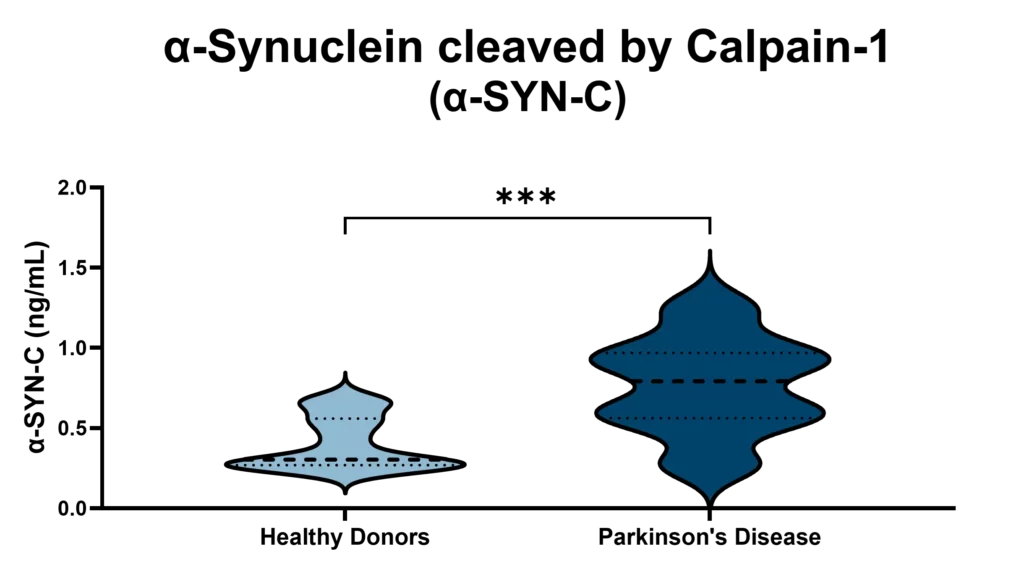
At Nordic Bioscience, we have developed an innovative approach to harness this biomarker potential. Using our ProteinFingerPrint Biomarker Technology™, we can detect Calpain-1-cleaved α-synuclein fragments in blood serum with high precision. Our specific assay, α-SYN-C, captures the unique “fragment fingerprint” of PD by quantifying these cleaved fragments, which are significantly elevated in the blood of PD patients compared to healthy individuals,as illustrated in Figure 2.
Figure 2. Patients with Parkinson’s Disease has significant higher levels of α-SYN-C in serum, compared to healthy donors. The α-SYN-C biomarker detects levels of α-Synuclein cleaved by Calpain-1 in serum. The assay is technically validated for measurements in human blood samples.
This biomarker offers a non-invasive, accessible tool for monitoring Parkinson’s Disease progression and evaluating therapeutic responses. By examining α-SYN-C levels in blood samples, our technology not only provides insights into PD mechanisms but also opens doors for developing targeted therapies that address the disease’s underlying pathology. Through this work, we aim to support more accurate PD diagnostics and more effective, individualized treatments in the fight against neurodegeneration.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
Hi-drad-uh-NIE-tis sup-yoo-ruh-TIE-vuh – also known as hidradenitis suppurutiva (HS) – is a pathologically complicated skin condition, where chronic skin inflammation leads to abscesses and scarring. It is a systemic disease with local manifestations, meaning that the chronic insult to the skin is systemic, but it is physically located where skin rubs against skin, such as the armpits, groins and under the breasts. It is well known that immune cells, such as neutrophils and mast cells are involved, but what do we know about tissue remodeling?
When the beautiful collagens of the skin become a part of disease pathogenesis
Patients with HS not only experience pain from the neutrophil-rich tunnels but also from excessive tissue remodeling that causes scarring of the skin. These patients have an imbalance in tissue formation and tissue repair, partly due to the excessive activity of immune cells, which release enzymes that degrade the skin.
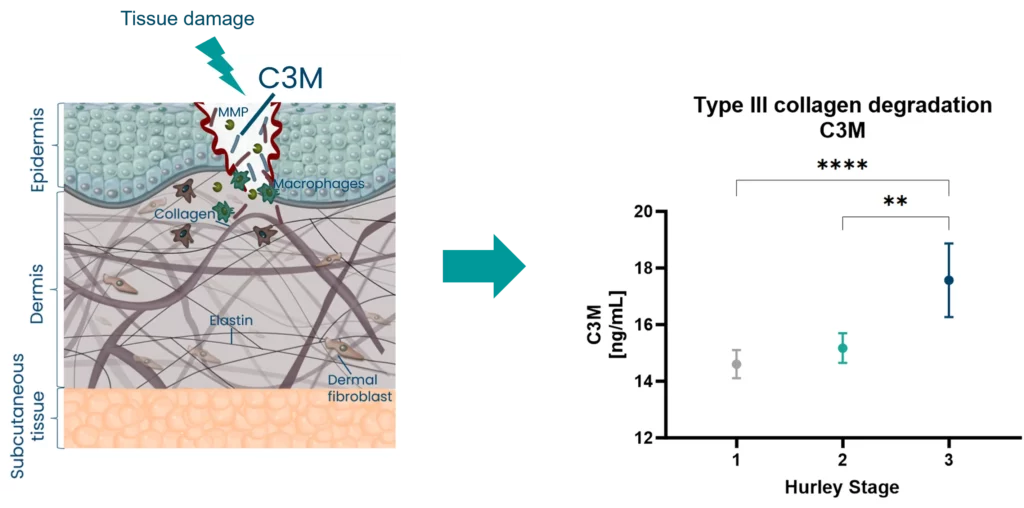
One group of tissue-degrading enzymes are matrix metalloproteinases, abbreviated as MMPs. These are released by macrophages, the most numerous inflammatory cells found in HS patients. MMPs infiltrate and contribute to HS pathology, signaling that increased activity of MMPs degrades the proteins of the skin tissue, such as collagens. This process can be quantified by specific blood-based biomarker assays targeting this pathological process.
Pathological fragments in HS may be used to identify disease types
In HS, biomarkers of tissue remodeling such as type III collagen degraded by MMPs (C3M), are associated with disease severity (Hurley Staging).
Figure 1. Biomarkers of tissue remodeling associate with Hurley Stages
C3M is released upon MMP activation and measures dermal tissue remodeling. This raises the question – can we use C3M to identify subtypes of patients based on their disease activity, and potentially molecular endotypes to help select the right treatment for the patients?
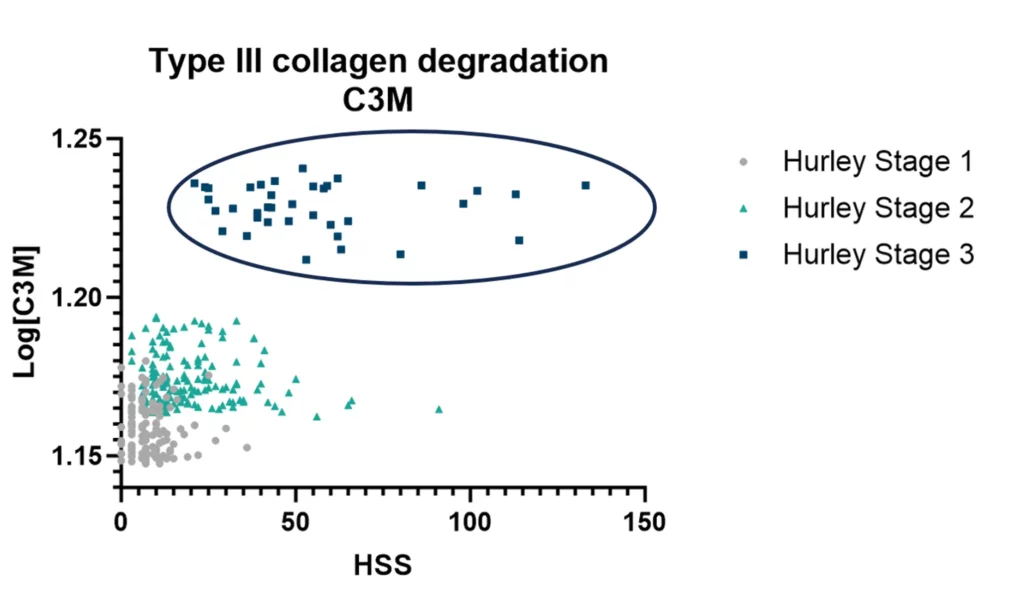
To address this, the levels of C3M are different depending on how active the disease is when divided into the Sartorious Score (HSS).
Finding the patients with high C3M levels reflects high disease activity, and may indicate a different subtype of patients needing a different treatment type.
Figure 2. Type II collagen degradation biomarker C3M as a patient stratification tool
Liver fibrosis is a progressive condition characterized by the excessive accumulation of scar tissue in the liver, often resulting from chronic liver diseases. Fibroblast activity plays a critical role in the progression of fibrosis, leading to organ function loss and liver-related complications. Liver fibrosis accounts for approximately 2 million deaths worldwide, while alcohol-related liver disease (ArLD) causes over 330,000 cirrhosis deaths globally every year.
In two recent studies, we investigated the fibrogenesis biomarker nordicPRO-C3™ in the context of advanced liver disease and full-spectrum fibrosis in alcohol-related liver disease. Our goal was to assess the nordicPRO-C3™ biomarker’s potential prognostic value and clinical utility as a predictor of outcome, and our results are very promising.
The nordicPRO-C3™ biomarker is capable of identifying advanced liver fibrosis and alcohol-related liver disease, providing a new clinical utility tool
In the first paper, published in JHEP Reports, we conducted investigations using two distinct cohorts of patients with compensated cirrhosis of mixed etiologies. In both cohorts, a 2-fold increase in nordicPRO-C3™ at baseline was associated with a significant hazard increase for liver-related events. Notably, nordicPRO-C3™ exhibited prognostic significance.
The identification of nordicPRO-C3™ as an independent prognostic factor for liver-related clinical outcomes has important implications for both drug development and clinical practice. By understanding the dynamic range of nordicPRO-C3™, researchers can improve its utility as a predictive marker in drug trials, enabling the development of targeted therapies to mitigate fibrosis progression and improve patient outcomes.
In a clinical setting, the integration of nordicPRO-C3™ measurement alongside established markers such as fibrosis-4 index (FIB-4) or transient elastography (TE) may enhance risk stratification and inform treatment decisions. Early identification of patients at higher risk for liver-related events can facilitate timely interventions, such as disease monitoring, lifestyle modifications, and appropriate therapeutic interventions.
In the second paper, published in Liver International, we assessed nordicPRO-C3™ models to predict liver-related events in patients with a history of excessive alcohol use but without a confirmed diagnosis of chronic liver disease. Our findings our promising for improving risk stratification and clinical outcomes in alcohol-related liver disease.
A prospective cohort study involving patients with alcohol-related Liver Disease (ArLD), was conducted and divided into a derivation cohort of secondary care patients and a validation cohort of primary care patients. Baseline variables, including nordicPRO-C3™, were utilized to develop a prediction model known as the ALPACA score. The prognostic accuracy of the ALPACA score was compared to existing tools such as the enhanced liver fibrosis (ELF) test, FIB-4, TE, and the ADAPT score (developed for fatty liver disease).
The ALPACA score demonstrated excellent discriminative accuracy in both the derivation and validation cohorts, comparable to TE and the ELF test, and superior to FIB-4, nordicPRO-C3™ alone, and the ADAPT score. Importantly, the ALPACA score provided reliable prognostic performance independent of the baseline fibrosis stage. This breakthrough has the potential to revolutionize risk stratification and patient management in primary and secondary care settings.
NordicPRO-C3™ has recently become available on the Roche-COBAS high-precision platform, paving the way for its commercial availability worldwide in the near future. This accessibility will enable widespread adoption of nordicPRO-C3™-based scores, leading to improved risk prediction and better outcomes for individuals.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
We have collected some of our best publications that we and our collaborators worked on in the second quarter of 2023—in no particular order. We invite you to browse and read according to your interests!
Hepatology
Alcohol-related liver disease (ArLD) leads to progressive liver-related outcomes and death, necessitating vigilant monitoring. Examining patients with ArLD over an average of 5.2 years, the PRO-C3-based score known as ALPACA (PRO-C3/AST/ALT, Platelets) demonstrated remarkable prognostic capability for liver-related events.
Comparatively, FIB-4, single markers like PRO-C3, ADAPT, ELF, and liver stiffness measures were all surpassed by the predictive efficacy of the ALPACA score in assessing outcomes for ArLD patients.
Fibronectin is a key protein for matrix organization and has been described as the glue of the extracellular matrix. The novel biomarker FN-EDB targets a degradation fragment of cellular fibronectin and showed to be elevated in patients with idiopathic pulmonary fibrosis.
This new biomarker enables quantification of a vital matrix embedded protein – laying the groundwork for important future studies.
In this study, we explored three collagen type III markers in the kidney’s interstitial matrix. These markers exhibited varied expressions and associations with inflammation, kidney function, and fibrosis in IgA nephropathy patients.
These findings emphasize the significance of selecting appropriate epitopes for distinct organs and diseases. Notably, urinary C3M emerges as a potential non-invasive fibrosis biomarker, complementing kidney biopsies in IgA nephropathy.
In our second renal publication, We examined whether collagen type III fragment C3M relates to inflammation markers and endothelial dysfunction, predicting chronic kidney disease (CKD) progression in type 2 diabetes patients with microalbuminuria.
Inflammatory markers and select endothelial indicators correlated with baseline serum C3M. Doubling serum C3M predicted CKD progression (accounting for mortality risk) post-conventional factor adjustment. These findings highlight serum C3M’s dual role as a CKD risk predictor and inflammation marker in type 2 diabetes.
Biomarkers aren’t just confined to different omics categories; various classes are referring to the types of serological measurements.
Consider cytokines, growth factors, receptors, kinases, transcription factors, intracellular proteins, extracellular proteins, and a subset within that—Extracellular Matrix (ECM) proteins. The common denominator in most pathologies is a loss of balance between different ECM proteins, especially collagens.
Biomarkers are more than just omics categories
This excessive destruction and deposition of proteins significantly propel the progression of end-stage diseases, culminating in organ dysfunction, failure, and, ultimately, death.
Diverse cytokines and growth factors orchestrating via specific receptors and kinases lead to ECM destruction and deposition, making ECM the converging pathway for multiple stimuli.
By the end of the day, what matters is to reverse ECM deterioration, or even undo, organ damage and function decline. Reversing organ damage can be achieved by stopping ECM deterioration. To truly reverse organ damage and restore organ functionality in patients, we need to repair the ECM to its normal balance.
We at Nordic Bioscience believe that the answer lies in effecting change at the tissue level—the key to reversing organ damage and, in turn, revitalizing organ function.
Have you considered if your treatment or pathway is affecting tissue formation or degradation? If so, feel free to browse our unique ECM biomarker portfolio.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
Nordic Bioscience’s extracellular matrix-based dermatology biomarkers offer a unique approach that sets them apart from competitors, providing deeper insights into tissue formation, degradation, immune cell activity, and resolution processes related to skin diseases. Unlike wide-range proteomics arrays, our biomarkers are fundamentally different and more specific, offering a higher level of clarity and precision.
Nordic Bioscience’s ECM-based dermatology biomarkers offer a unique approach
A clear connection
The clear connection between our dermatology biomarkers and skin diseases lies in the fact that immune cell activity, skin tissue remodeling and genetic mutations of collagens are known to cause these conditions. By identifying pathology specific biomarkers, we not only indicate the presence of a disease in a patient but also highlight the local manifestation of an underlying systemic cause. This genetic link and visible manifestation on the skin create a relatable narrative for stakeholders and pharmaceutical companies, potentially paving the way towards a better understanding of the disease.
A key advantage of our skin disease biomarkers is the limited competition in the market, and no approved biomarkers for skin diseases. With no competitors in the tissue-based biomarker space, we have the opportunity to position ourselves as leaders in this area. Supported by compelling data that demonstrates pathology specificity, disease activity, disease progression, and pharmacodynamic response, there is a rare chance for pharmaceutical partners to be among the first movers and pioneers in this field.
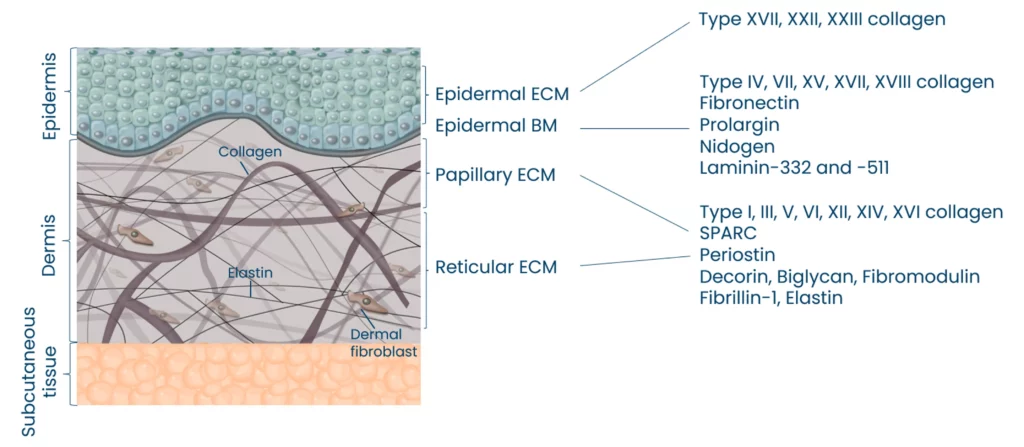
Moreso, we have observed that skin aging and cross-linking collagens are correlated. Our biomarkers can quantify the age of collagens by measuring alpha and beta CTX-III together with the ECM of the epidermis and dermis.
Nordic Bioscience can quantify specific pathological fragments from the different compartments of the skin
Implications for precision medicine
Precision medicine is a crucial aspect empowered by our dermatology biomarkers. By providing information about ongoing pathological processes within the tissue, such as damage and repair, we enable targeted treatments and therapies that enhance patient outcomes. This personalized medicine approach is far more effective than relying on proteomic providers’ hope of hitting the right target by chance. Our markers aid in drug development by specifically identifying target populations and reducing costs, ultimately expediting the development process.
Our skin disease biomarkers play a vital role in elucidating the mechanism of action (MoA) of treatments. Here, we can also shed light on the speed at which a compound modulates tissue and fibroblast derived biomarkers, providing essential information on the efficacy and responsiveness of the treatment.
Furthermore, by analyzing the objective disease activity, we can determine how the compound affects specific factors associated with the patient’s profile, such as neutrophil activity, mast cell activity, macrophage activity, soft tissue destruction, systemic fibroblast activity, and more. This holistic evaluation enables a deeper understanding of how the compound influences different aspects of the disease process, ultimately facilitating the development of more effective and targeted therapies for patients.
Robust technology
Our laboratory technology is robust and meets CLSI validation guidelines, ensuring reliability and accuracy. Moreover, our derma markers can be seamlessly integrated into Roche automated platforms, making them easily accessible worldwide. This scalability and dependability are vital for the development of reliable clinical research tools, further solidifying the value of our biomarkers in the field of dermatology.
A potential case for melanoma studies
While our dermatology markers have broad applicability, there is a particularly intriguing potential use in melanoma. By understanding the tissue formation, degradation, and repair processes specific to this type of skin cancer, we can offer valuable insights for diagnosis and management.
For clients involved in ongoing metastatic melanoma research, we can help establish a connection between extracellular matrix remodeling and melanoma, positioning our biomarkers as a valuable resource for further investigation and improving patient care.
Nordic Bioscience’s ECM-based biomarkers provide a relatable and comprehensive narrative by connecting genetic links, visible skin manifestations, and in-depth insights into ongoing pathological processes. With unparalleled clarity and understanding, our biomarkers empower precision medicine in skin diseases. Supported by robust technology, validated methodologies, and a potential application in melanoma, our biomarkers offer an unprecedented opportunity for stakeholders and pharmaceutical companies.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
In the field of clinical trials, accuracy and reliability are critical to success. For this reason, Nordic Bioscience Laboratory is dedicated to providing the highest quality laboratory services, with a strong focus on data integrity, customer satisfaction, and scientific excellence.
Our clinical laboratory offers central lab and specialty lab services, including a wide range of diagnostic and exploratory tests that are essential for meeting patients’ care needs and advancing drug development efforts. We use state-of-the-art equipment and technology, as well as a team of highly skilled laboratory professionals, to deliver fast, accurate and reliable results without sacrificing quality.
Nordic Bioscience Clinical Laboratory offers central and specialty lab services
Compliance at every step of the way
We pride ourselves on ensuring that biomarker validation complies with European Medicines Agency (EMA) and Food and Drug Administration (FDA) guidelines. In addition, we provide access to a team of scientific experts who have the experience and expertise to help you navigate the complexities of biomarker research, interpret data, and make informed decisions about your studies.
Our Clinical Laboratory is accredited by the College of American Pathologists (CAP) and all aspects of laboratory services are performed in accordance with international Good Clinical Practice (GCP) and Good Clinical laboratory Practices (GCLP) standards. Our accreditation reflects our unwavering commitment to providing the highest quality laboratory services that adhere to the most rigorous industry standards.
Commitment to improvement
As part of our ongoing commitment to continuous improvement, our processes, and procedures are regularly reviewed and audited by numerous external auditors and accreditation bodies. These audits enable us to continuously improve and innovate our laboratory services to meet the latest regulatory requirements. We also invest in the continuous education and training of our staff to stay abreast of the latest laboratory science. These efforts allow us to maintain our high-quality standards and ensure that our customers receive the best possible laboratory services, as well as scientific excellence that can help them interpret data.
At Nordic Bioscience Laboratory, we hold ourselves to the highest standard of quality and place a high value on providing a personalized experience for clinical testing. We are committed to serving as your trusted partner in delivering accurate and reliable laboratory services that help advance the field of clinical trials.
We hope that you will consider partnering with Nordic Bioscience for your clinical laboratory needs. We look forward to the opportunity to work with you and support your research activities.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
Collagen is a crucial protein that provides structural support and strength to tissues throughout the body. However, there is a group of highly specialized minor collagens that may play a critical role in cancer progression. Most research on the biology of collagens has focused on the abundant collagens, but the highly specialized minor collagens that are expressed only at certain developmental stages may be deregulated in cancer.
The Hypothesis
Minor collagens are widely expressed during embryogenesis, as they organize the extracellular matrix (ECM) to support tissue development. However, in adult tissues, minor collagens become restricted to a few specific organs and are expressed at very low levels.
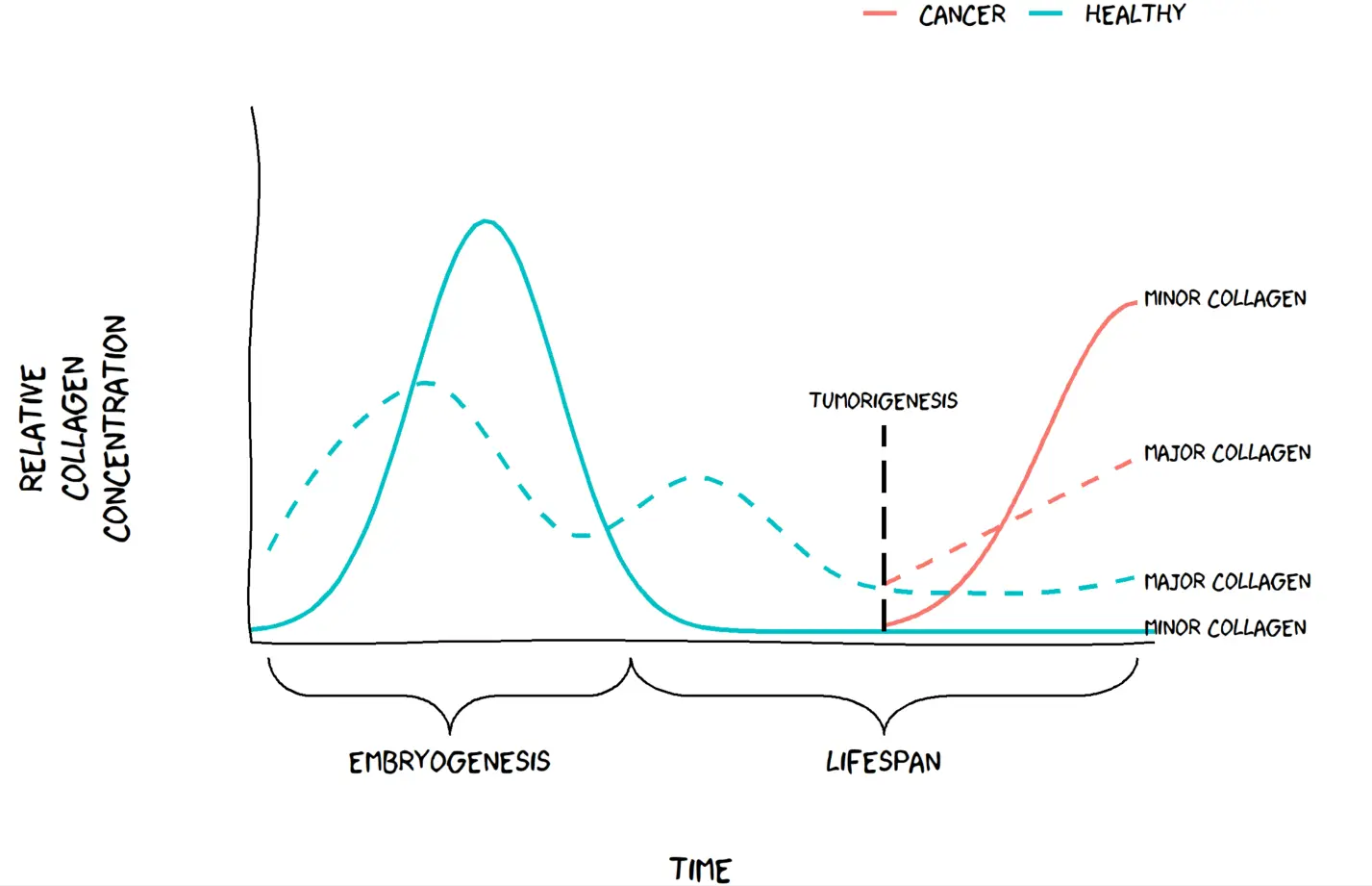
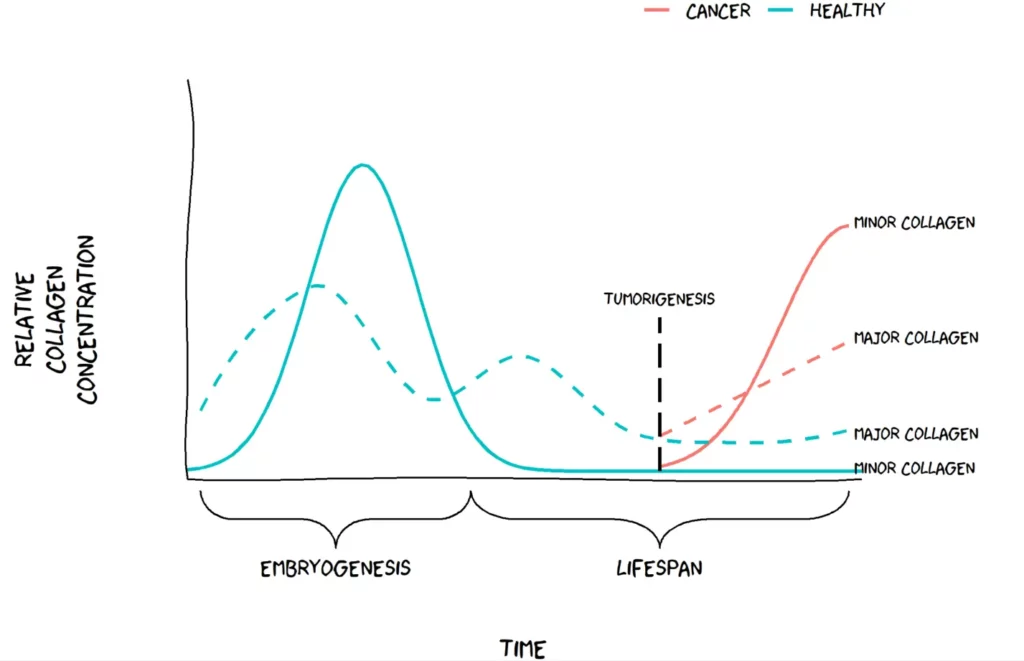
Recent studies have suggested that minor collagens may become deregulated in cancer, where they are highly upregulated in tumor tissues. This upregulation is thought to occur as the ECM is reorganized during tumor development and progression. We have chosen to call this hypothesis “The Minor Collagen Hypothesis”. We hypothesize that minor collages, which are normally restricted to embryonic tissues, may become active again in adult tissues as cancer progresses. The Minor Collagen Hypothesis proposes that this reactivation may be a key component in in tumor growth and invasion by altering the composition of the ECM.
Visualization of the minor collagen hypothesis. Figure by Jeppe Thorlacius-Ussing.
Applying The Minor Collagen Hypothesis in clinical research
Biomarkers are important for indicating the presence or severity of a disease, and in cancer, they are crucial for early detection, monitoring of cancer progression, and guiding treatment decisions.
In general, several collagen biomarkers are overexpressed in cancer. However, minor collagens may offer a more specific biomarker for certain types of cancer. For example, recent research has shown that certain subtypes of cancer-associated fibroblasts (CAFs) express specific minor collagens. These collagens can be detected in blood, making them potential targets for drug development aimed at CAFs.
This hypothesis offers researchers new possibilities and highlights the need for more specific biomarkers for cancer diagnosis and treatment that could lead to better patient outcomes. Identifying biomarkers that detect specific minor collagens could be a breakthrough in cancer research and might shed light on an overlooked aspect of cancer progression.
Minor collagens are typically expressed during embryogenesis or tissue development and are expressed at low levels afterward. In cancer, however, these specialized collagens are expressed again to form an environment conducive to cancer growth. The abundant major collagens are also expressed during tissue development and growth spurts in childhood and adolescence but tapers off in adulthood. The relative induction as a function of cancer is greater for the minor collagens compared to the major collagens. This could mean better biomarker performance.
Understanding Fibrosis Remodeling in Animal Models
Animal testing is a crucial aspect of drug development, mandated by the FDA for all premature drugs in development. However, a critical question arises: how can we be sure that the pathology observed in rodents is reflective of the same pathology in humans? This is a significant concern for the medical community because of the potential for negative consequences if clinical trials are based on inaccurate preclinical data as we see in humans. Why then is it so important to measure biomarker formations in rodents? Because it matters whether it mimics the right pathology.
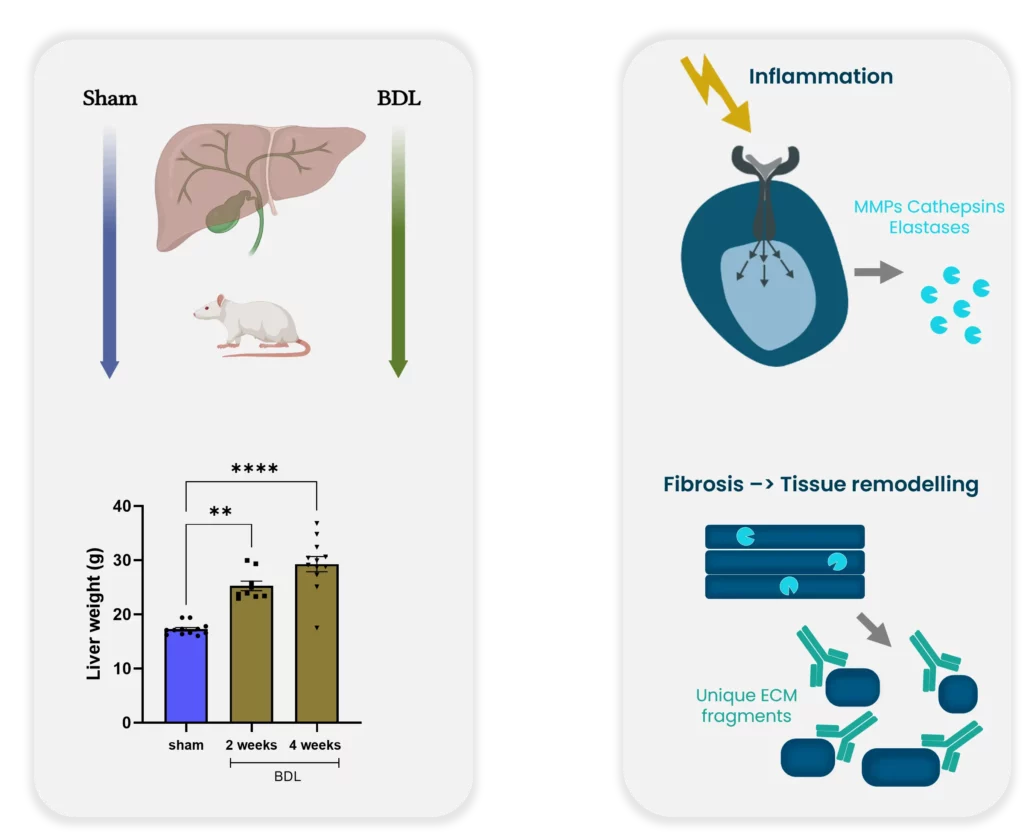
Example for bridging preclinical and clinical practice. Bile duct ligation: a preclinical model of liver fibrosis.
The process of transitioning from preclinical to clinical trials is critical to success. Histological stages are built on human tissue sections and used for comparison to create an appropriate animal model. However, none of the existing rodent models currently develop nonalcoholic steatohepatitis (NASH) as seen in humans. This discrepancy raises concerns regarding the usefulness of rodent models for preclinical studies.
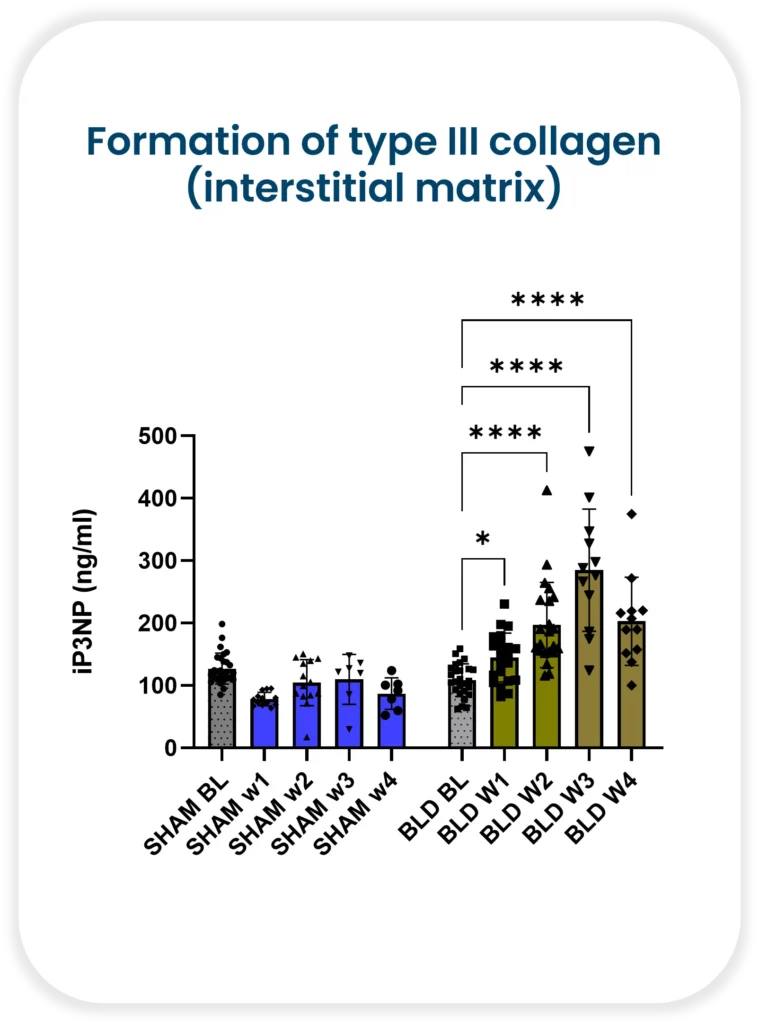
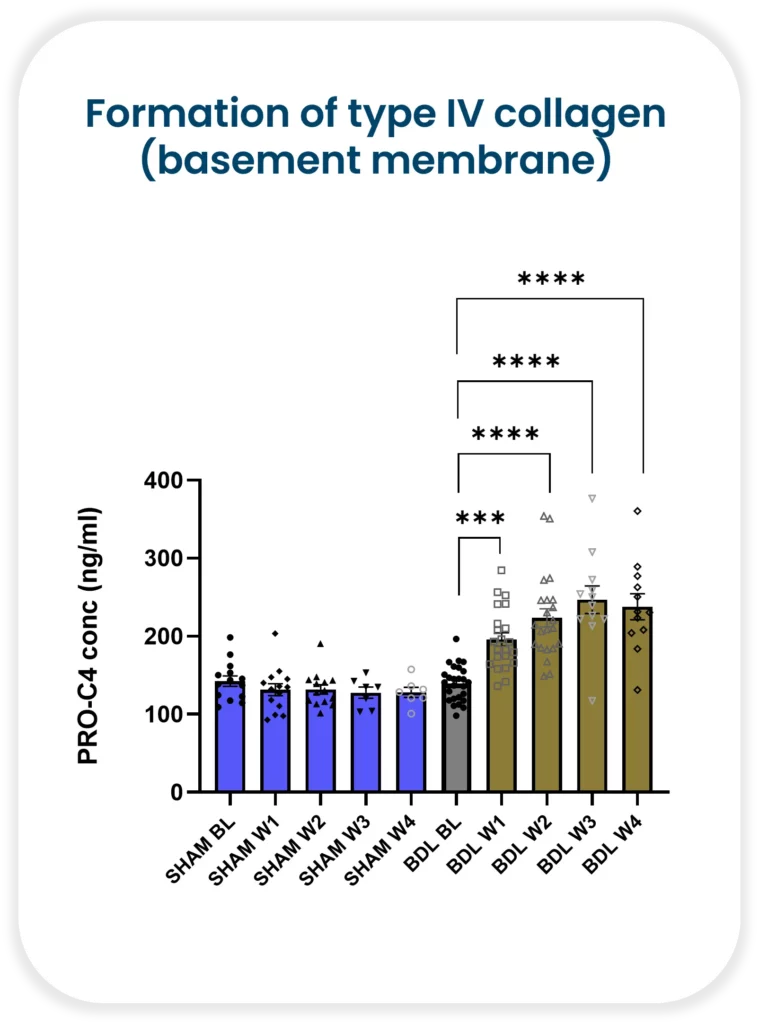
Despite these concerns, it is still essential to measure biomarker formations in rodents. The reason being, it matters whether the biomarker mimics the correct pathology. Nordic Bioscience has demonstrated increasing formation of both type III collagen (interstitial matrix) and type IV collagen (basement membrane) with continued injury in a rat bile duct ligation model. Collagen III has been shown to be upregulated in human liver fibrosis, including NASH, and is associated with increased severity. On the other hand, collagen IV is a measure of early fibrosis remodeling.
Bile duct ligation: a preclinical model of liver fibrosis
It is critical to understand fibrosis remodeling during disease progression in both animals and humans. With Nordic Bioscience’s biomarkers, researchers can improve translation between the preclinical and clinical practice. The use of biomarkers enables researchers to track disease progression and evaluate the effectiveness of potential treatments accurately. Moreover, they can also help identify patients who are likely to respond positively to a particular therapy.
Animal testing remains a critical aspect of drug development, it is essential to understand rodent model limitations. Biomarkers offer an effective way to track the progression of disease accurately. We can identify patients likely to benefit from a specific treatment and improve the transition from preclinical to clinical trials. By leveraging biomarkers in both animal and human models, we can make sure that the right therapy is provided to the right patient—at the right time.


 The
The