Biomarkers aren’t just confined to different omics categories; various classes are referring to the types of serological measurements.
Consider cytokines, growth factors, receptors, kinases, transcription factors, intracellular proteins, extracellular proteins, and a subset within that—Extracellular Matrix (ECM) proteins. The common denominator in most pathologies is a loss of balance between different ECM proteins, especially collagens.
Biomarkers are more than just omics categories
This excessive destruction and deposition of proteins significantly propel the progression of end-stage diseases, culminating in organ dysfunction, failure, and, ultimately, death.
Diverse cytokines and growth factors orchestrating via specific receptors and kinases lead to ECM destruction and deposition, making ECM the converging pathway for multiple stimuli.
By the end of the day, what matters is to reverse ECM deterioration, or even undo, organ damage and function decline. Reversing organ damage can be achieved by stopping ECM deterioration. To truly reverse organ damage and restore organ functionality in patients, we need to repair the ECM to its normal balance.
We at Nordic Bioscience believe that the answer lies in effecting change at the tissue level—the key to reversing organ damage and, in turn, revitalizing organ function.
Have you considered if your treatment or pathway is affecting tissue formation or degradation? If so, feel free to browse our unique ECM biomarker portfolio.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
Nordic Bioscience’s extracellular matrix-based dermatology biomarkers offer a unique approach that sets them apart from competitors, providing deeper insights into tissue formation, degradation, immune cell activity, and resolution processes related to skin diseases. Unlike wide-range proteomics arrays, our biomarkers are fundamentally different and more specific, offering a higher level of clarity and precision.
Nordic Bioscience’s ECM-based dermatology biomarkers offer a unique approach
A clear connection
The clear connection between our dermatology biomarkers and skin diseases lies in the fact that immune cell activity, skin tissue remodeling and genetic mutations of collagens are known to cause these conditions. By identifying pathology specific biomarkers, we not only indicate the presence of a disease in a patient but also highlight the local manifestation of an underlying systemic cause. This genetic link and visible manifestation on the skin create a relatable narrative for stakeholders and pharmaceutical companies, potentially paving the way towards a better understanding of the disease.
A key advantage of our skin disease biomarkers is the limited competition in the market, and no approved biomarkers for skin diseases. With no competitors in the tissue-based biomarker space, we have the opportunity to position ourselves as leaders in this area. Supported by compelling data that demonstrates pathology specificity, disease activity, disease progression, and pharmacodynamic response, there is a rare chance for pharmaceutical partners to be among the first movers and pioneers in this field.
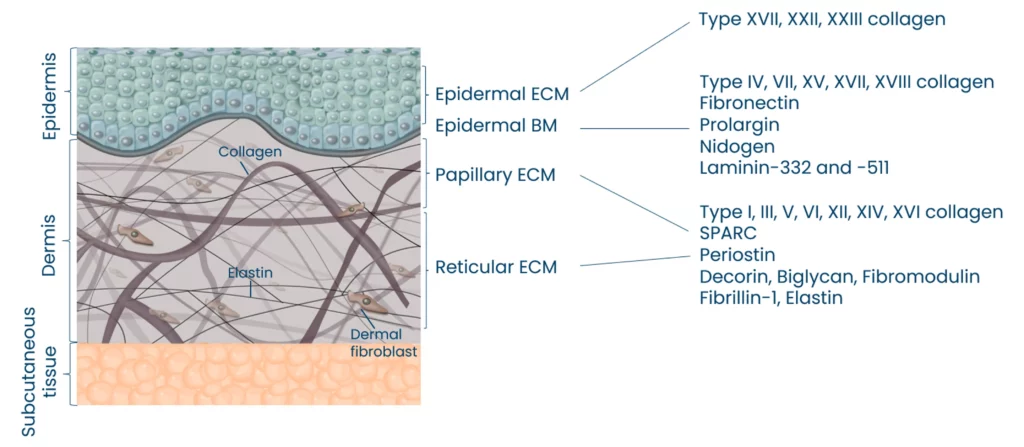
Moreso, we have observed that skin aging and cross-linking collagens are correlated. Our biomarkers can quantify the age of collagens by measuring alpha and beta CTX-III together with the ECM of the epidermis and dermis.
Nordic Bioscience can quantify specific pathological fragments from the different compartments of the skin
Implications for precision medicine
Precision medicine is a crucial aspect empowered by our dermatology biomarkers. By providing information about ongoing pathological processes within the tissue, such as damage and repair, we enable targeted treatments and therapies that enhance patient outcomes. This personalized medicine approach is far more effective than relying on proteomic providers’ hope of hitting the right target by chance. Our markers aid in drug development by specifically identifying target populations and reducing costs, ultimately expediting the development process.
Our skin disease biomarkers play a vital role in elucidating the mechanism of action (MoA) of treatments. Here, we can also shed light on the speed at which a compound modulates tissue and fibroblast derived biomarkers, providing essential information on the efficacy and responsiveness of the treatment.
Furthermore, by analyzing the objective disease activity, we can determine how the compound affects specific factors associated with the patient’s profile, such as neutrophil activity, mast cell activity, macrophage activity, soft tissue destruction, systemic fibroblast activity, and more. This holistic evaluation enables a deeper understanding of how the compound influences different aspects of the disease process, ultimately facilitating the development of more effective and targeted therapies for patients.
Robust technology
Our laboratory technology is robust and meets CLSI validation guidelines, ensuring reliability and accuracy. Moreover, our derma markers can be seamlessly integrated into Roche automated platforms, making them easily accessible worldwide. This scalability and dependability are vital for the development of reliable clinical research tools, further solidifying the value of our biomarkers in the field of dermatology.
A potential case for melanoma studies
While our dermatology markers have broad applicability, there is a particularly intriguing potential use in melanoma. By understanding the tissue formation, degradation, and repair processes specific to this type of skin cancer, we can offer valuable insights for diagnosis and management.
For clients involved in ongoing metastatic melanoma research, we can help establish a connection between extracellular matrix remodeling and melanoma, positioning our biomarkers as a valuable resource for further investigation and improving patient care.
Nordic Bioscience’s ECM-based biomarkers provide a relatable and comprehensive narrative by connecting genetic links, visible skin manifestations, and in-depth insights into ongoing pathological processes. With unparalleled clarity and understanding, our biomarkers empower precision medicine in skin diseases. Supported by robust technology, validated methodologies, and a potential application in melanoma, our biomarkers offer an unprecedented opportunity for stakeholders and pharmaceutical companies.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
In the field of clinical trials, accuracy and reliability are critical to success. For this reason, Nordic Bioscience Laboratory is dedicated to providing the highest quality laboratory services, with a strong focus on data integrity, customer satisfaction, and scientific excellence.
Our clinical laboratory offers central lab and specialty lab services, including a wide range of diagnostic and exploratory tests that are essential for meeting patients’ care needs and advancing drug development efforts. We use state-of-the-art equipment and technology, as well as a team of highly skilled laboratory professionals, to deliver fast, accurate and reliable results without sacrificing quality.
Nordic Bioscience Clinical Laboratory offers central and specialty lab services
Compliance at every step of the way
We pride ourselves on ensuring that biomarker validation complies with European Medicines Agency (EMA) and Food and Drug Administration (FDA) guidelines. In addition, we provide access to a team of scientific experts who have the experience and expertise to help you navigate the complexities of biomarker research, interpret data, and make informed decisions about your studies.
Our Clinical Laboratory is accredited by the College of American Pathologists (CAP) and all aspects of laboratory services are performed in accordance with international Good Clinical Practice (GCP) and Good Clinical laboratory Practices (GCLP) standards. Our accreditation reflects our unwavering commitment to providing the highest quality laboratory services that adhere to the most rigorous industry standards.
Commitment to improvement
As part of our ongoing commitment to continuous improvement, our processes, and procedures are regularly reviewed and audited by numerous external auditors and accreditation bodies. These audits enable us to continuously improve and innovate our laboratory services to meet the latest regulatory requirements. We also invest in the continuous education and training of our staff to stay abreast of the latest laboratory science. These efforts allow us to maintain our high-quality standards and ensure that our customers receive the best possible laboratory services, as well as scientific excellence that can help them interpret data.
At Nordic Bioscience Laboratory, we hold ourselves to the highest standard of quality and place a high value on providing a personalized experience for clinical testing. We are committed to serving as your trusted partner in delivering accurate and reliable laboratory services that help advance the field of clinical trials.
We hope that you will consider partnering with Nordic Bioscience for your clinical laboratory needs. We look forward to the opportunity to work with you and support your research activities.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
Collagen is a crucial protein that provides structural support and strength to tissues throughout the body. However, there is a group of highly specialized minor collagens that may play a critical role in cancer progression. Most research on the biology of collagens has focused on the abundant collagens, but the highly specialized minor collagens that are expressed only at certain developmental stages may be deregulated in cancer.
The Hypothesis
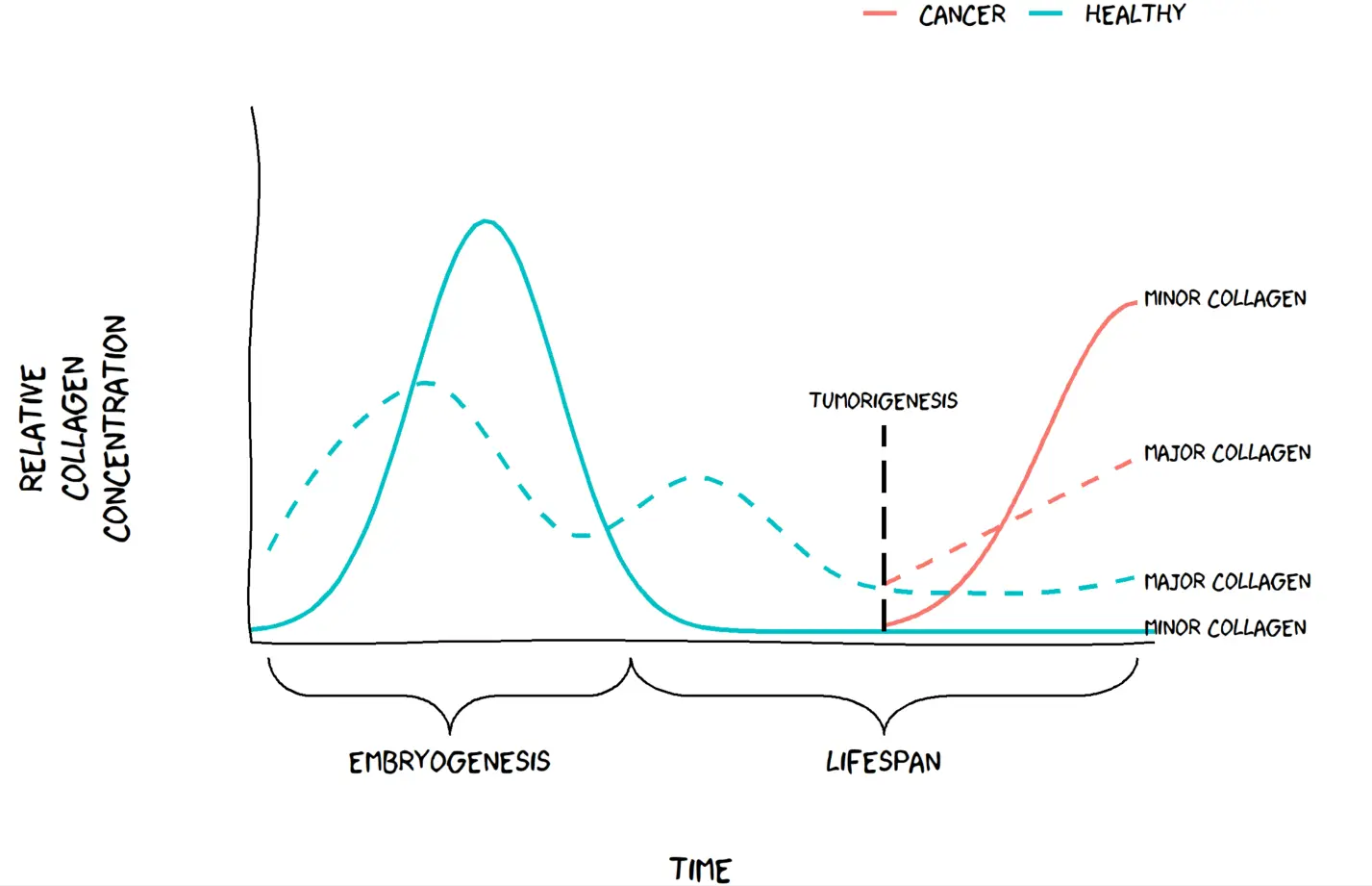
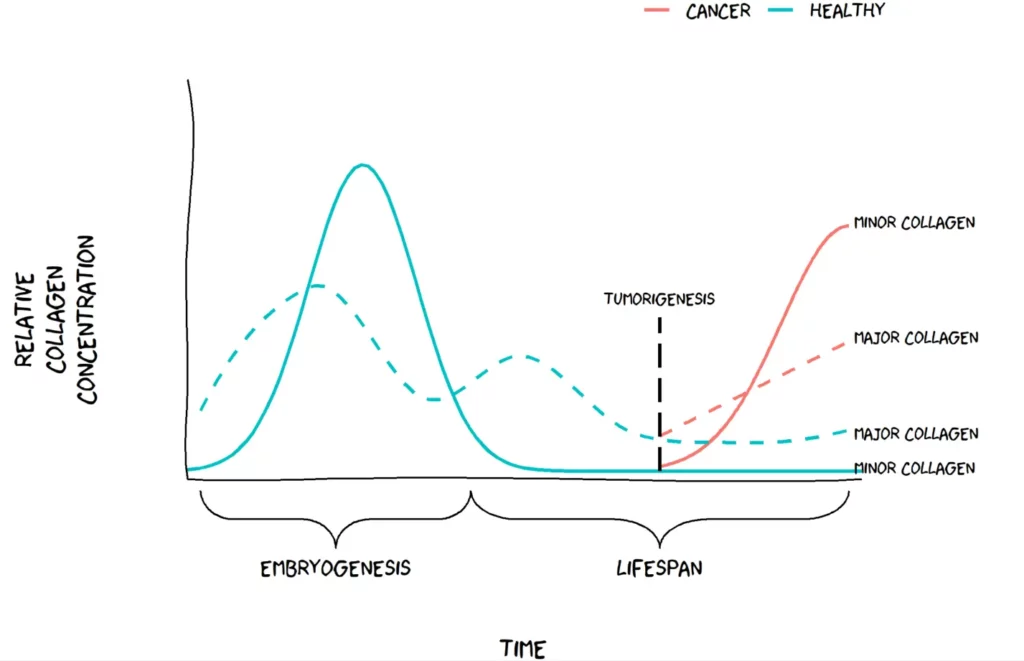
Minor collagens are widely expressed during embryogenesis, as they organize the extracellular matrix (ECM) to support tissue development. However, in adult tissues, minor collagens become restricted to a few specific organs and are expressed at very low levels.
Recent studies have suggested that minor collagens may become deregulated in cancer, where they are highly upregulated in tumor tissues. This upregulation is thought to occur as the ECM is reorganized during tumor development and progression. We have chosen to call this hypothesis “The Minor Collagen Hypothesis”. We hypothesize that minor collages, which are normally restricted to embryonic tissues, may become active again in adult tissues as cancer progresses. The Minor Collagen Hypothesis proposes that this reactivation may be a key component in in tumor growth and invasion by altering the composition of the ECM.
Visualization of the minor collagen hypothesis. Figure by Jeppe Thorlacius-Ussing.
Applying The Minor Collagen Hypothesis in clinical research
Biomarkers are important for indicating the presence or severity of a disease, and in cancer, they are crucial for early detection, monitoring of cancer progression, and guiding treatment decisions.
In general, several collagen biomarkers are overexpressed in cancer. However, minor collagens may offer a more specific biomarker for certain types of cancer. For example, recent research has shown that certain subtypes of cancer-associated fibroblasts (CAFs) express specific minor collagens. These collagens can be detected in blood, making them potential targets for drug development aimed at CAFs.
This hypothesis offers researchers new possibilities and highlights the need for more specific biomarkers for cancer diagnosis and treatment that could lead to better patient outcomes. Identifying biomarkers that detect specific minor collagens could be a breakthrough in cancer research and might shed light on an overlooked aspect of cancer progression.
Minor collagens are typically expressed during embryogenesis or tissue development and are expressed at low levels afterward. In cancer, however, these specialized collagens are expressed again to form an environment conducive to cancer growth. The abundant major collagens are also expressed during tissue development and growth spurts in childhood and adolescence but tapers off in adulthood. The relative induction as a function of cancer is greater for the minor collagens compared to the major collagens. This could mean better biomarker performance.
Understanding Fibrosis Remodeling in Animal Models
Animal testing is a crucial aspect of drug development, mandated by the FDA for all premature drugs in development. However, a critical question arises: how can we be sure that the pathology observed in rodents is reflective of the same pathology in humans? This is a significant concern for the medical community because of the potential for negative consequences if clinical trials are based on inaccurate preclinical data as we see in humans. Why then is it so important to measure biomarker formations in rodents? Because it matters whether it mimics the right pathology.
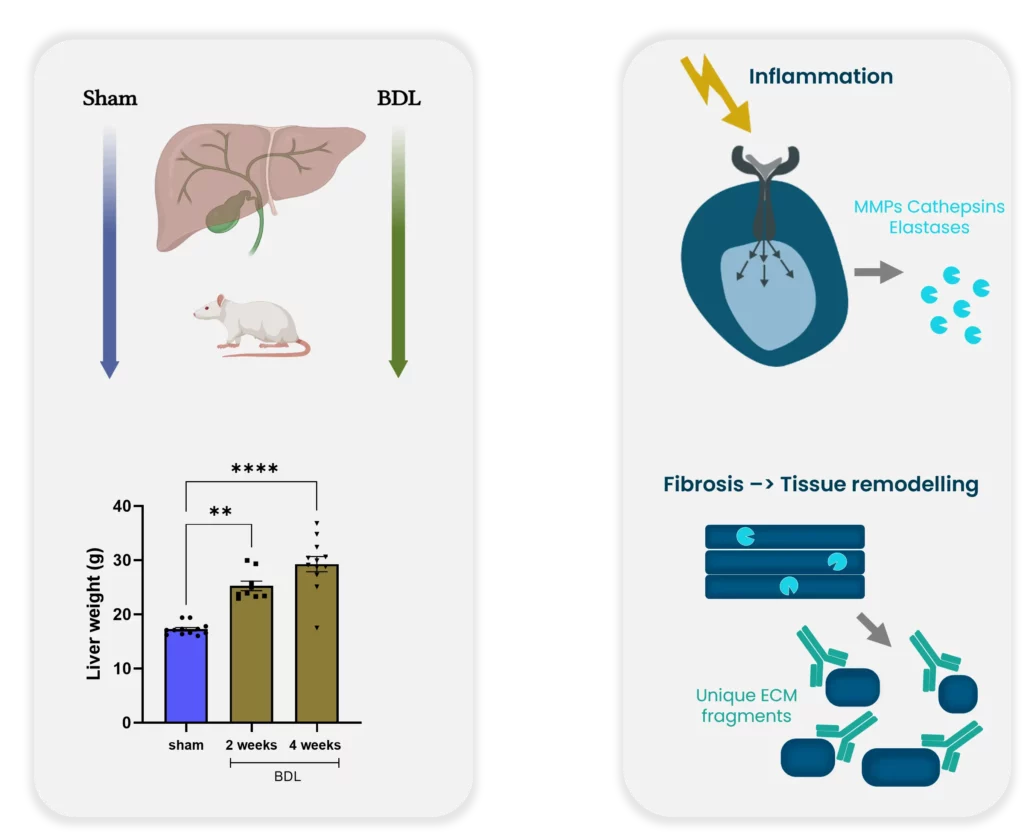
Example for bridging preclinical and clinical practice. Bile duct ligation: a preclinical model of liver fibrosis.
The process of transitioning from preclinical to clinical trials is critical to success. Histological stages are built on human tissue sections and used for comparison to create an appropriate animal model. However, none of the existing rodent models currently develop nonalcoholic steatohepatitis (NASH) as seen in humans. This discrepancy raises concerns regarding the usefulness of rodent models for preclinical studies.
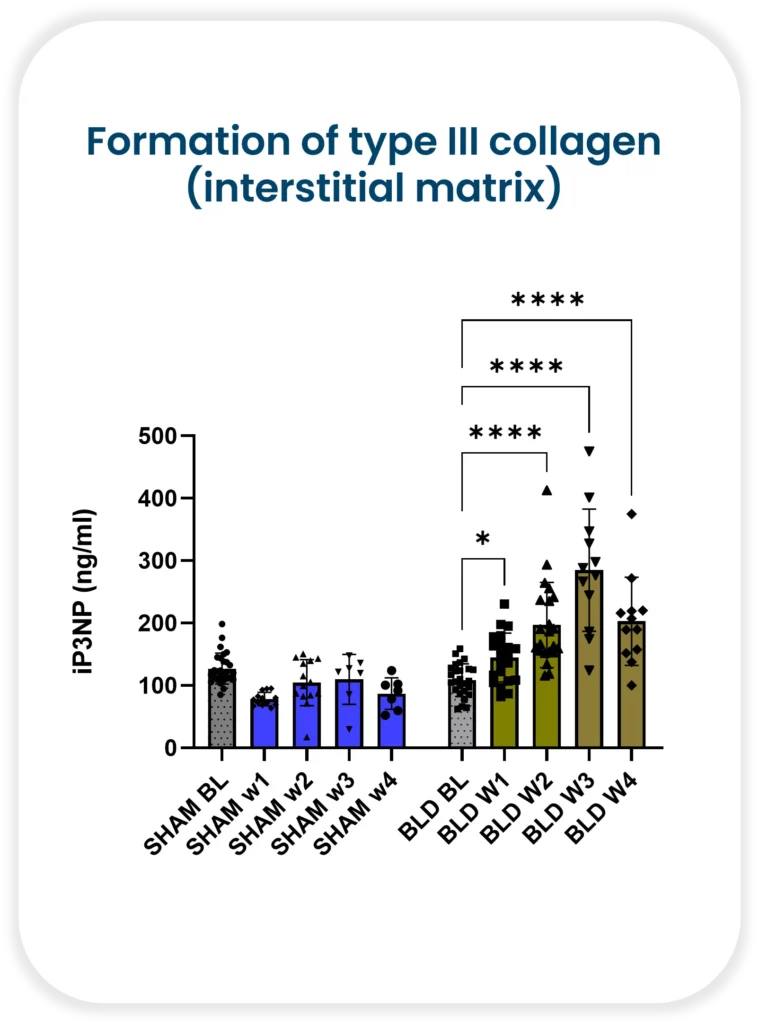
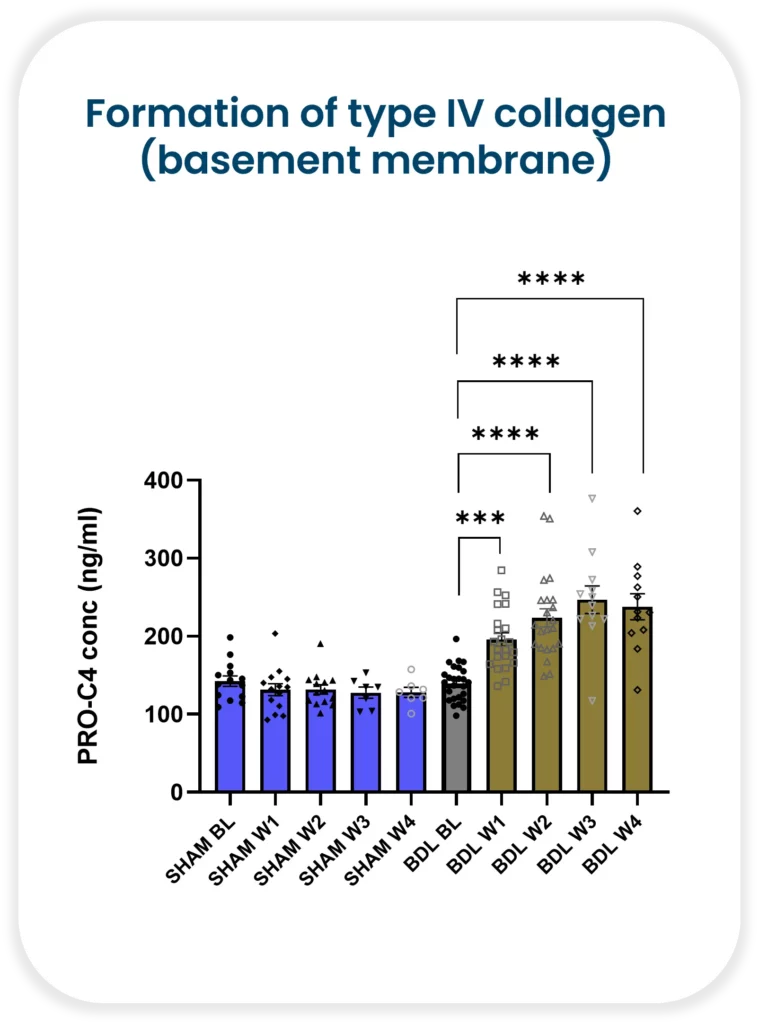
Despite these concerns, it is still essential to measure biomarker formations in rodents. The reason being, it matters whether the biomarker mimics the correct pathology. Nordic Bioscience has demonstrated increasing formation of both type III collagen (interstitial matrix) and type IV collagen (basement membrane) with continued injury in a rat bile duct ligation model. Collagen III has been shown to be upregulated in human liver fibrosis, including NASH, and is associated with increased severity. On the other hand, collagen IV is a measure of early fibrosis remodeling.
Bile duct ligation: a preclinical model of liver fibrosis
It is critical to understand fibrosis remodeling during disease progression in both animals and humans. With Nordic Bioscience’s biomarkers, researchers can improve translation between the preclinical and clinical practice. The use of biomarkers enables researchers to track disease progression and evaluate the effectiveness of potential treatments accurately. Moreover, they can also help identify patients who are likely to respond positively to a particular therapy.
Animal testing remains a critical aspect of drug development, it is essential to understand rodent model limitations. Biomarkers offer an effective way to track the progression of disease accurately. We can identify patients likely to benefit from a specific treatment and improve the transition from preclinical to clinical trials. By leveraging biomarkers in both animal and human models, we can make sure that the right therapy is provided to the right patient—at the right time.
CPa9-HNE ELISA has emerged as a novel serum calprotectin biomarker
Status quo: Crohn’s and Colitis biomarkers
Conventional serum calprotectin biomarkers are often not as clinically useful as the fecal versions, which is related to the half-life of calprotectin in blood (only 5-6 hours), leading to dissociation of calprotectin protein. The short half-life of calprotectin in blood reduces the window in which the current serum calprotectin ELISA assay can detect calprotectin dimer protein, which is composed of monomers S100A8 and S100A9.
By applying the Protein Fingerprint technology, we have identified a neo-epitope of the S100A9 monomer of calprotectin derived from proteolytic cleavage by human neutrophil elastase (HNE). This ELISA assay is referred to as the CPa9-HNE assay and is a new and innovative method for quantification of calprotectin in serum developed by Nordic Bioscience.
Inflammatory Bowel Disease (IBD) flares in the intestines.
A new tool to measure… calprotectin
Patients with Crohn’s disease and ulcerative colitis have been found to show significantly higher levels of CPa9-HNE in their serum than healthy subjects, with the AUC reaching 0.98 (CI: 0.97-1.00, p<0.0001) for CD and 0.96 (CI: 0.92-1.00, p<0.0001) for UC, proving the assay’s efficacy in distinguishing between disease states.
In comparison, the MRP8/14 serum calprotectin assay from Bühlmann Lab, while also used to identify IBD, showed poorer separation between patients and healthy subjects, with AUCs of 0.72 (CI: 0.59-0.86, p=0.0025) for UC and 0.70 (CI: 0.56-0.84, p=0.0046) for CD, respectively.
The CPa9-HNE biomarker showed a better correlation with the endoscopic score for Crohn’s disease (SES-CD) and ulcerative colitis (MES) than the FCP. At the same time, the MRP8/14 assay and neutrophil count showed no significant correlation with endoscopic scores for IBD patients.
To investigate the accuracy of the CPa9-HNE, we performed a received operator characteristic curve, demonstrating CPa9-HNE with acceptable accuracy to identify patients with IBD in remission vs. active disease.
Finally, we demonstrated that the CPa9-HNE biomarker could detect the calprotectin neo-epitope only in the supernatant of in vitro activated primary human neutrophils, but not in inactive primary human neutrophils. This was in contrast to the MRP8/14 serum CP assay of the Bühlmann lab, as both inactive and activated primary human neutrophils secreted detectable levels of calprotectin.
CPa9-HNE ELISA proved to be a novel serum calprotectin biomarker with significant clinical potential as a biomarker for patients with IBD to monitor disease activity and neutrophil activity.
However, circulating calprotectin metabolites released from locally inflamed mucosa are not be dissociated further. They can be readily quantified using an ELISA-based technique called Protein Fingerprint technology. This refined ELISA technique quantifies protein metabolites or neo-epitopes derived from proteolysis that reflect local tissue inflammation and remodeling.
PRO-C6 Findings In NEJM Evidence to Help Patient Segregation in HFpEF
A persistent problem remains a challenge in HFpEF – patient heterogeneity.
We need the right patients for the right treatment, but how do we get it to them? We believe that one approach to solving this problem is to improve patient segregation and endotyping.
In collaboration with Bristol Myers Squibb and University of Pennsylvania, we recently identified a subset of patients at a very high risk of adverse outcomes, all characterized by increased fibroblast activity. Using our PRO-C6 biomarker assay we can accurately quantify this risk profile and differentiate patients based on how likely they are to be re-hospitalized or have all-cause mortality due to heart failure.
These findings were recently published in NEJM Evidence.
So how do we deal with patient heterogeneity?
We believe it is time to give physicians and clinicians a better tool than what is available now.
This is endotrophin endotyping, heart failure risk stratification redefined.
Get in touch
Are you interested in exploring collaboration possibilities? Enter your information in the form and a representative will contact you shortly.
We need to talk about the good and the bad fibroblasts – the dangerous fibroblasts that overgrow organs and destroy organ function, but also the necessary specialized fibroblasts in bone, the osteoblasts.
Fibroblasts are an important type of cell in the human body that play a crucial role in tissue repair and maintenance. However, not all fibroblasts are created equal – there are both good and bad fibroblasts that have vastly different effects on the body.
The dangerous fibroblasts, known as myofibroblasts, are responsible for pathological tissue remodeling in various diseases, such as fibrosis. These fibroblasts overgrow organs and destroy organ function. While myofibroblasts play a role in wound healing, their persistence and unchecked growth can lead to excessive scarring and tissue damage.
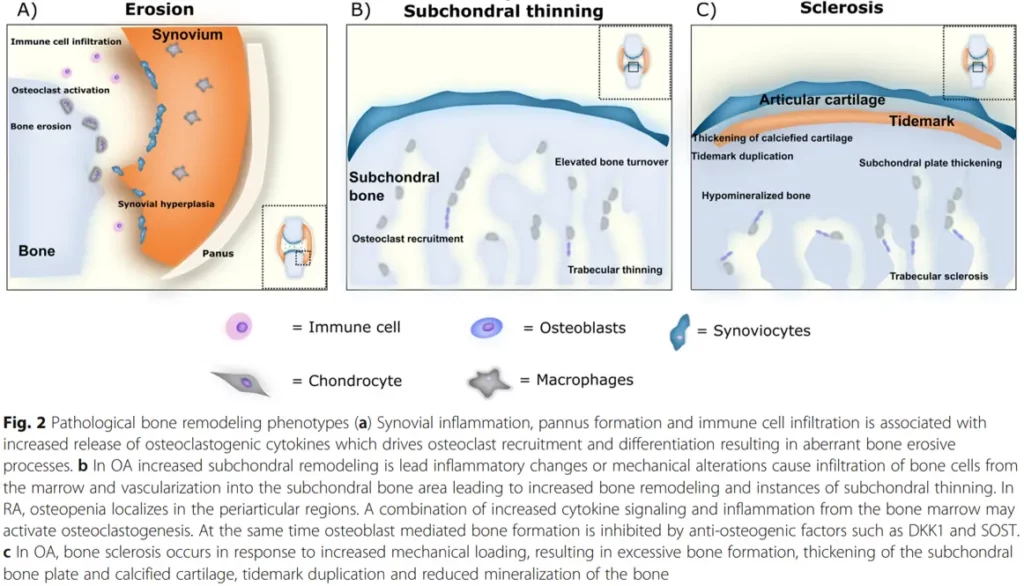
Pathological bone remodeling phenotypes
On the other hand, there are specialized fibroblasts, such as osteoblasts, that are necessary for maintaining bone health. Osteoblasts are responsible for producing the extracellular matrix that makes up bone tissue, and are crucial in the process of bone formation.
Unfortunately, the success in biomedical sciences such as genomics and proteomics is not paralleled in the medical product development methods, resulting in a lack of translation into improved drug safety and efficacy. This can lead to some antifibrotic treatments having deleterious effects on bone fibroblasts, such as osteoblasts, and may cause unwanted side effects.
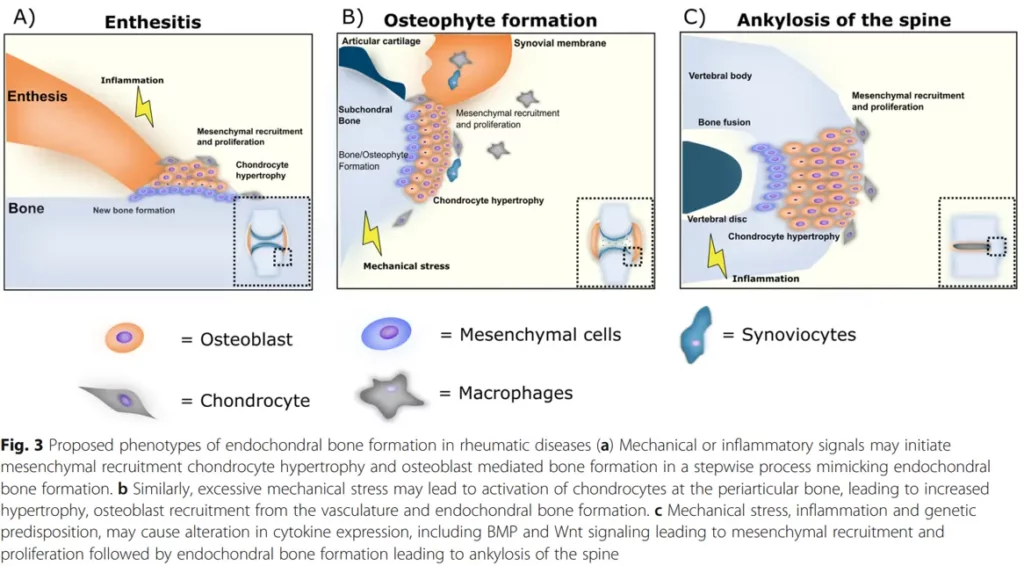
Proposed phenotypes of endochondral bone formation in rheumatic diseases
In rheumatic diseases, bone inflammation and remodeling phenotypes are proposed to be a result of endochondral bone formation. Studies have identified bone as a possible endocrine organ, and the availability of valid biochemical bone markers suggests that assessing bone turnover should also play an important role in general safety pharmacology.
To address this issue, there is a need for improved methods to assess the effects of treatments on different types of fibroblasts. This is where bone inflammation panels come in – these panels can be used to assess whether a treatment is having a deleterious effect on bone fibroblasts, such as osteoblasts.
In conclusion, while fibroblasts play a crucial role in tissue repair and maintenance, it is important to distinguish between the good and bad fibroblasts. Unchecked growth of myofibroblasts can lead to tissue damage and organ dysfunction, while osteoblasts are necessary for maintaining bone health. Improved methods of assessing the effects of treatments on different types of fibroblasts, such as bone inflammation panels, can help ensure that treatments are safe and effective.
With our bone inflammation panel, you can assess whether your treatment is having a deleterious effect.
The affect on the collagen microenvironment in breast cancer patients
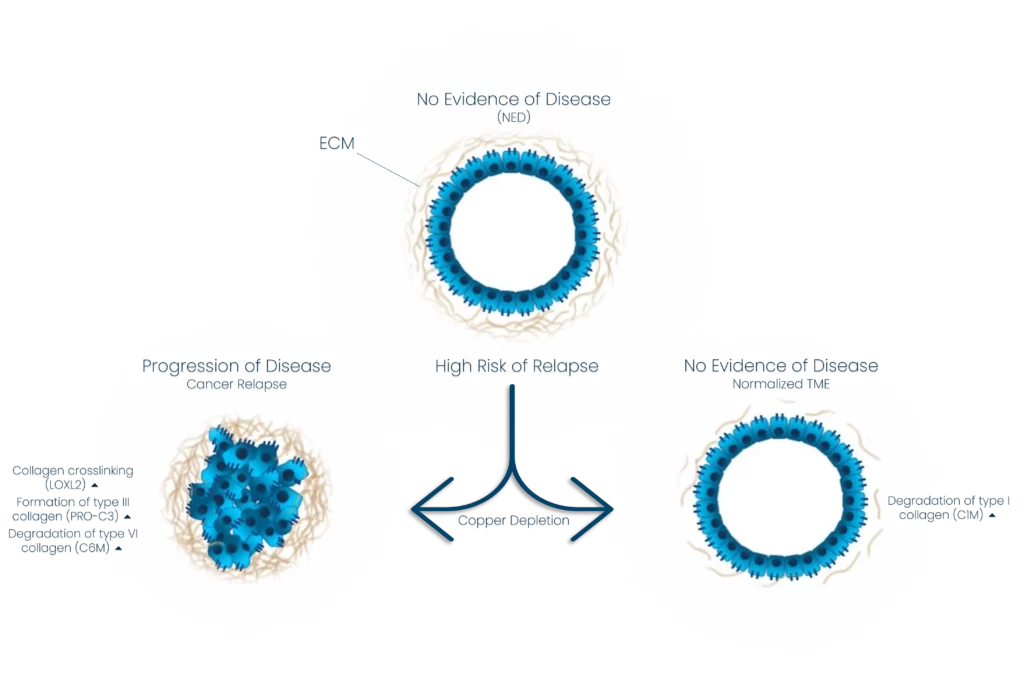
In a recently published study based on a collaboration between Nordic Bioscience, Memorial Sloan Kettering Cancer Center, Weill Cornell Medicine, and Nancy E. and Peter C. Meinig School of Biomedical Engineering, we have examined the effect of copper depletion therapy on the collagen microenvironment in breast cancer patients with a high risk of relapse.
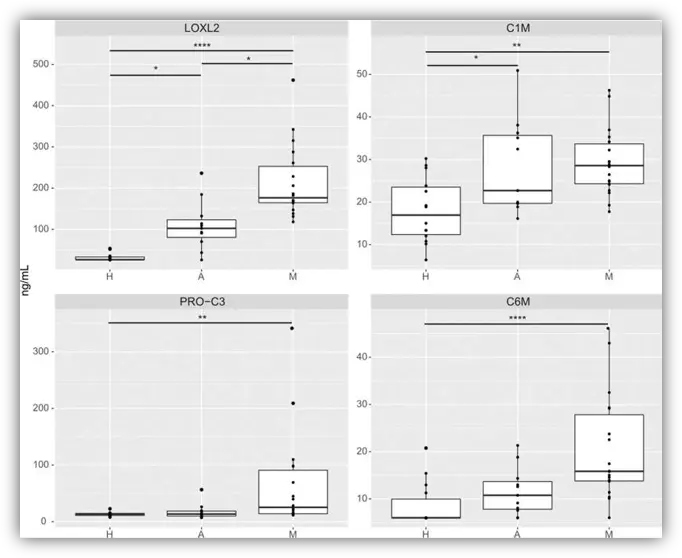
Tetrathiomolybdate (TM) is a novel, copper-depleting compound associated with promising survival in a phase II study of patients with high-risk and triple-negative breast cancer. In the study, levels of all collagen biomarkers were higher in those with the disease, metastatic and adjuvant, as compared with healthy controls.
Baseline biomarkers of collagen crosslinking (LOXL2), collagen formation (PRO-C3), and collagen degradation (C1M and C6M) in the exploratory cohort
We propose a novel mechanism for preventing metastases through altered collagen processing in the tumor microenvironment. We hypothesize that decreased collagen cross-linking and increased degradation caused by the treatment may alter the immune response in the pre-metastatic sites and thereby decrease the metastatic potential.
The effect of copper depletion therapy on collagen turnover in breast cancer patients
Preclinical studies revealed decreased collagen deposition, lower levels of myeloid-derived suppressor cells, and higher CD4+ T-cell infiltration in TM-treated mice compared with controls.
In conclusion, the study showed novel mechanisms of TM targeting the TME and immune response with potential applications across cancer types.
Autosomal dominant polycystic kidney disease (ADPKD) is a hereditary condition that causes the development of cysts in the kidneys. This condition affects millions of people worldwide and can lead to kidney failure if left untreated. One of the biggest challenges in treating ADPKD is identifying biomarkers that can predict disease progression and response to treatment.
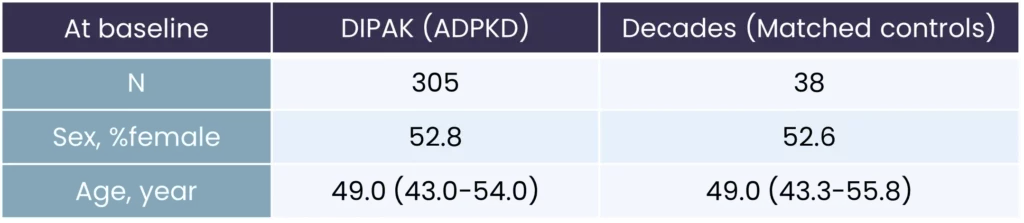
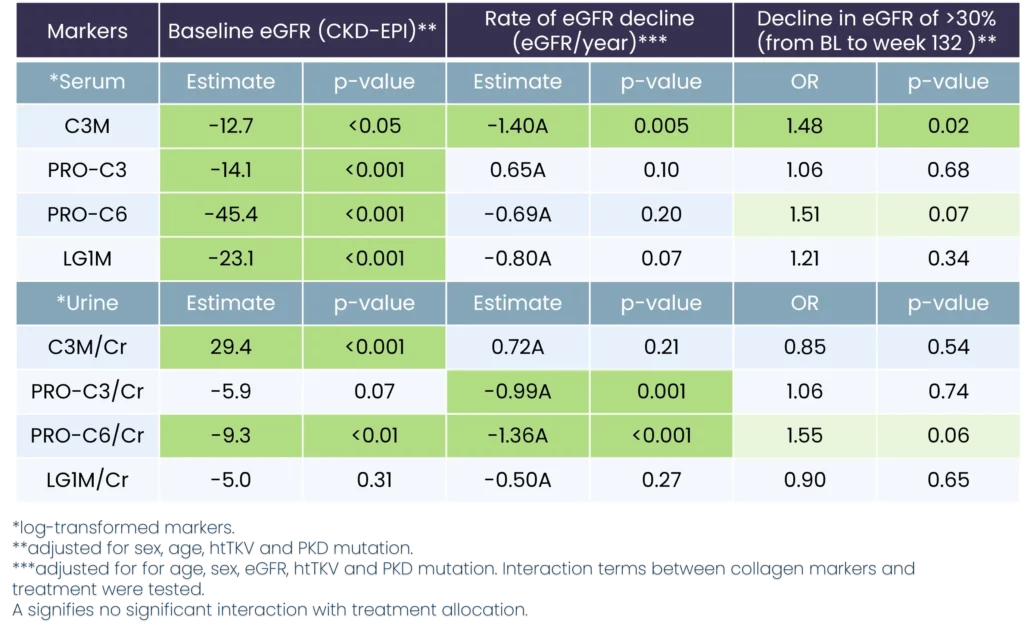
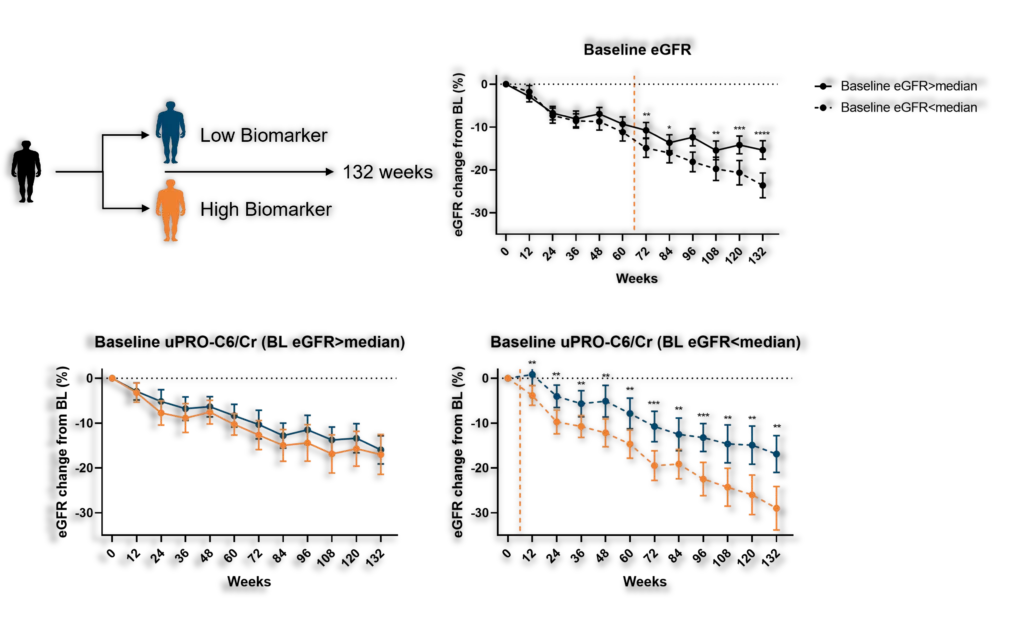
Our Renal and Cardiovascular Research team showed that biomarkers of collagen remodeling measured in urine and circulation at baseline are associated with the rate of decline in kidney function in patients with ADPKD. In the study (DIPAK-1), we measured the effect of lanreotide on patients with stage 3 chronic kidney disease. The following demographics were involved:
DIPAK-1 demographics
To assess the effect of lanreotide, the team selected a number of biomarkers that were best suited to assess the effect of the drug on interstitial matrix turnover and basement membrane turnover. We have selected a number of biomarkers:
PRO-C3, measuring collagen type III formation in serum and urine (interstitial matrix turnover)
C3M, measuring collagen type III degradation in serum and urine (interstitial matrix turnover)
PRO-C6, measuring collagen type VI formation in serum and urine. Also measures the release of the bioactive fragment endotrophin, associated with pro-fibrotic and pro-inflammatory processes (interstitial matrix turnover)
LG1M, measuring Laminin gamma 1 degradation in serum and urine (basement membrane turnover)
Kidney biomarker data compared to baseline values
Predicting decline in kidney function with prognostic biomarkers
The data we found implies that fibrogenesis may be an important pathophysiological process driving ADPKD disease progression. In addition, the use and development of drugs that interfere with fibrogenesis may be promising to halt disease progression in ADPKD. However, we still need to validate in an independent cohort, preferably in early-stage disease.
The findings of the study are significant because they offer new insights into the potential for biomarkers to predict disease progression in ADPKD. This information may help clinicians to identify patients who are at risk of developing kidney failure and to develop more effective treatments to slow or halt disease progression.
We have shown that biomarkers of collagen remodeling are associated with the rate of decline in kidney function in patients with ADPKD. These findings suggest that fibrogenesis may be an important pathophysiological process driving ADPKD disease progression and that the use of drugs that interfere with fibrogenesis may be promising to halt disease progression. Further research is needed to validate these findings in an independent cohort, but the results of this study offer new hope for patients with ADPKD.
We believe it is time to put kidney fibrosis more in the center – even in diseases where other aspects (such as kidney volume) are the focus of attention. At Nordic Bioscience, we have the tools to do so.