A recent analysis published in JAMA highlights a major epidemiological shift: Colorectal cancer (CRC) is now the leading cause of cancer-related death among adults under 50 in the United States.
CRC has long been perceived as a disease of older populations. The rapid rise in early-onset cases challenges that assumption and reinforces the need to rethink both biology and treatment strategies.
Why standard therapies still fall short: the fibrotic stroma as a resistance mechanism
Therapeutically, the backbone remains surgery in localized disease, combination chemotherapy regimens such as FOLFOX and FOLFIRI, anti-VEGF or anti-EGFR targeted therapies in selected patients, and immunotherapy in MSI-high/dMMR tumors. While these approaches have extended survival, resistance and relapse remain frequent, particularly in advanced disease.
One key and often underestimated driver of progression and resistance is fibrosis. CRC tumors are embedded in a collagen-rich, fibrostenotic microenvironment shaped by cancer-associated fibroblasts (CAFs). This dense extracellular matrix (ECM) does not merely provide structure. It represents a desmoplastic barrier that limits drug penetration, reduces treatment efficacy, and supports tumor progression.
From biology to measurement: collagen remodeling biomarkers
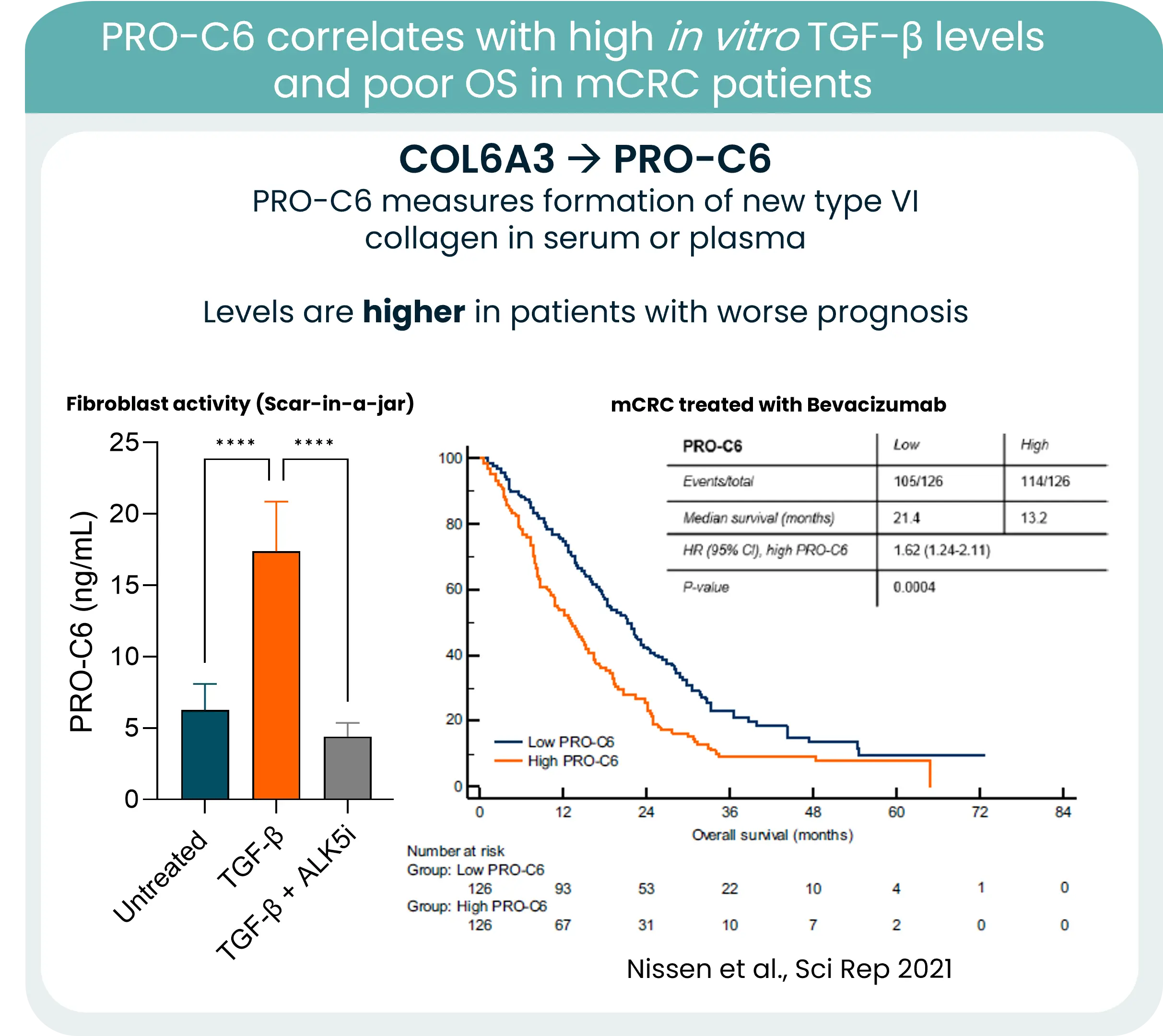
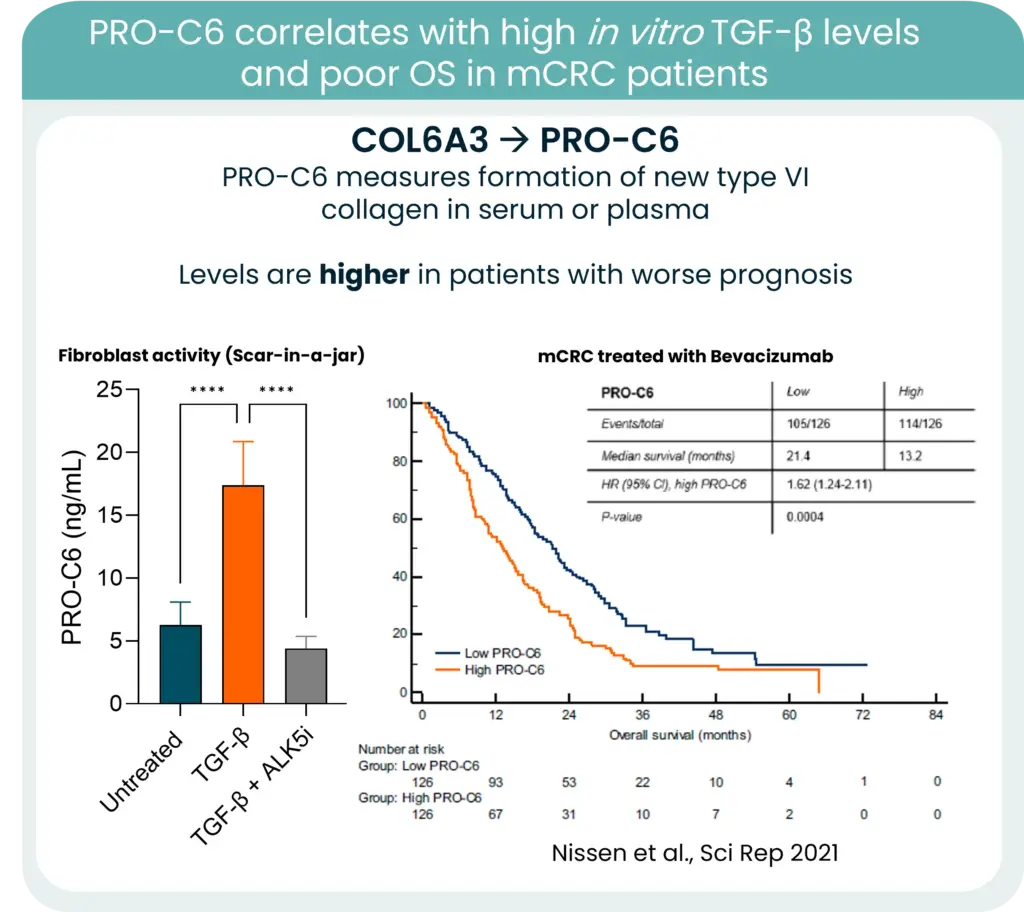
Collagens are central components of this barrier, and increased collagen deposition and remodeling consistently associate with poorer outcomes. One notable example is type VI collagen. Its gene expression is strongly associated with KRAS mutations and high TGF-β levels in CRC. New type VI collagen formation releases protein fragments to the bloodstream, which can be quantified in serum using our PRO-C6 biomarker and correlate to high TGF-β levels and poor OS.
In this context, measuring collagen formation and degradation becomes highly relevant. Quantifying ECM remodeling can provide insight into tumor aggressiveness, stromal activation, and potentially treatment response.
As early-onset CRC continues to rise, integrating stromal blood-based biomarkers into clinical strategy may refine risk stratification and open new opportunities for stroma-targeted interventions.
The future of CRC management will not rely solely on targeting tumor cells. It will require understanding and measuring the fibrotic environment that sustains them.